


 Kate Gunthorpe MPS[/caption]
Kate Gunthorpe MPS[/caption]
 Madison Low[/caption]
Madison Low[/caption]

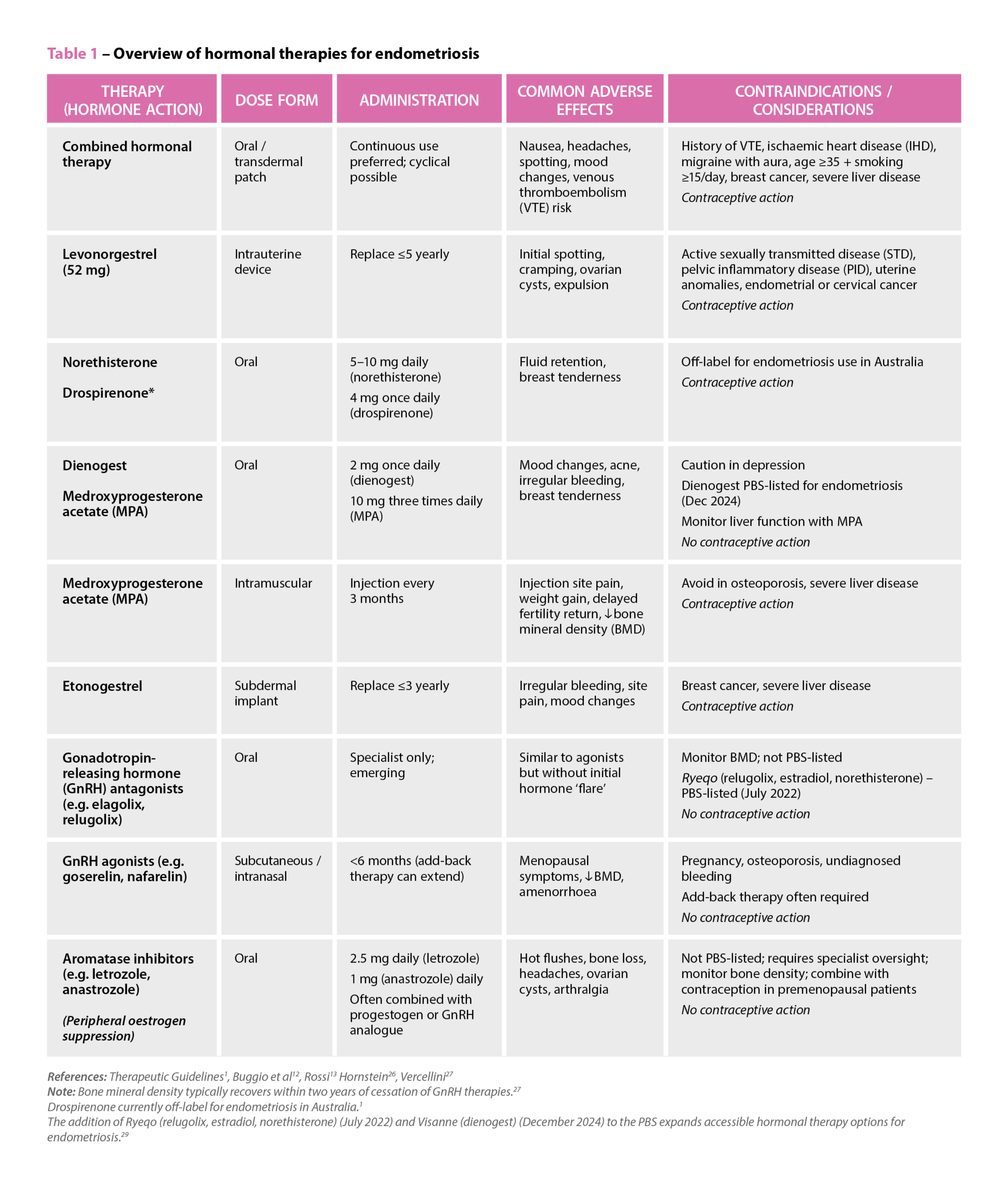 References: Therapeutic Guidelines
References: Therapeutic Guidelines

 Genevieve Adamo MPS (Image: Steve Christo Photography)[/caption]
Genevieve Adamo MPS (Image: Steve Christo Photography)[/caption]

The gap between evidence and everyday practice is impacting patient access to emergency contraception.
Community pharmacies are often the first – and sometimes only – point of access for emergency contraception in Australia.
But a new qualitative study found there are still persistent gaps between what the guidelines say and what happens in practice.
Ruth Nona, pharmacist and researcher at James Cook University, who interviewed community pharmacists about providing emergency contraception services, describes a workforce that is broadly willing to help, but not always set up to deliver consistently equitable care.
1. Not recommending ulipristal as first-line
One of the most significant gaps identified in the study was the tendency for pharmacists to default to levonorgestrel, despite guidance in the Australian Pharmaceutical Formulary and Handbook (APF) that ulipristal acetate is generally considered more effective than levonorgestrel and can be used up to 120 hours after unprotected intercourse.
‘Habit definitely plays a role,’ Ms Nona said. ‘Some pharmacists felt more comfortable and confident supplying levonorgestrel. For example, if someone requested emergency contraception within 24 hours, pharmacists felt levonorgestrel was acceptable within that timeframe, without fully considering efficacy.’

In some pharmacies, price differences influenced whether ulipristal acetate was presented as an option.
‘In certain socio-economic areas, cost was a driver,’ Ms Nona said. ‘Cost considerations were also sometimes linked to younger people coming in and asking whether there was a cheaper option.’
Sometimes, levonorgestrel was the only medicine on hand.
‘There was research that came out showing that some pharmacies still did not stock ulipristal acetate,’ she said. ‘It’s been an ongoing issue, and something that really needs to be addressed.’
However, patients need to be able to make an informed decision about which medicine to take.
‘As stated in the guidelines, it’s about making sure all patients are given the information they need to make an informed and equitable choice. If the patient wants a particular option, that’s fine, but they need to be able to make that decision with the full information,’ Ms Nona said.
‘When pharmacists did give the full picture and explained the differences, more often than not the patient chose ulipristal acetate, even though it cost more.’
‘If the patient wants a particular option, that’s fine, but they need to be able to make that decision with the full information.’
Ruth nona
2. Uncertainty when responding to third-party requests
Pharmacists reported particular uncertainty when providing emergency contraception to third parties, with many wary about consent and unsure whether they could provide it to someone who wasn’t the patient.
‘In most cases, they would follow up and ask to contact the patient directly,’ Ms Nona said. ‘It wasn’t that they didn’t want to provide it – they just felt unsure and they wanted to make sure that the patient had consented.’
While in many cases, speaking to the intended person directly can help provide key information and counselling, in circumstances where this is not possible, it is usually possible to determine the medicine is safe and therapeutically appropriate, and supply in a manner consistent with APF guidance and legal obligations.
3. Uncertainty providing emergency contraception to adolescents
Similarly, pharmacists were ‘uncomfortable’ providing the service to adolescents.
This uncertainty often centred on fear of making the wrong decision or facing professional consequences.
‘They still wanted to provide the service, but it was more that internal question of, “Should I do this? Am I going to get in trouble?”’
There are no jurisdictions where there’s a legal restriction from supplying emergency contraception to minors. The APF guidance helps pharmacists navigate Gillick competency and consent in adolescents, ensuring they demonstrate sufficient maturity and understanding to provide informed consent.
Ms Nona emphasised that the issue was confidence, not capability.
‘It’s about being familiar with the guidelines, making sure we’re as up to date as possible and realising that it’s okay for us to provide these services, provided the adolescent is [assessed as Gillick competent] mentally mature and safe,’ she said.
The APF references Gillick competency provided the adolescent is [assessed as Gillick competent (demonstrating sufficient maturity and understanding to provide informed consent)]
4. Uncertainty for transgender people on gender affirming hormone therapy
While pharmacists were generally supportive towards transgender and gender-diverse patients, lack of familiarity with hormone therapy raised hesitation.
‘There are absolutely no interactions between emergency contraception and gender-affirming hormones’ Ms Nona said. ‘It really comes down to knowledge, which builds confidence, and being up to date to make sure the service we provide is timely and equitable.’
In some areas, pharmacists may frequently encounter transgender and gender- diverse patients requesting emergency contraception, while pharmacists in other areas do not.
‘That’s why it’s also about being prepared. You never know when that situation might arise,’ she added.
Should pharmacists feel unsure during these consultations, pharmacists can and should engage with the APF.
‘Pharmacists did say that if that situation did occur with a transgender or gender- diverse person that they would be honest and say to them, “Do you mind if I consult my resources?”’
Another reason the APF is a mandatory text for all community pharmacists
Despite lack of guideline use, pharmacists acknowledged how essential guidelines
such as the APF are, Ms Nona said.
‘And when pharmacists did use them, they found the information provided was invaluable.’
‘[But] a lot of the challenges stemmed from lack of time and, in some cases, a lack of up-to-date knowledge. We have so many things to do, and we need more time to do everything and to keep ourselves up to date.’
For Ms Nona, the solution lies in supporting pharmacists to use guidelines confidently and consistently in real-world conditions.
Some pharmacists report to PSA that they will often bring up the APF digital on the screen in the consultation room in emergency contraception discussions, particularly in situations which are new or unfamiliar.
Delivering a critical intervention
The key to emergency contraception provision is recognising the stakes.
‘The whole picture of providing emergency contraception is to make sure we are preventing pregnancies when people don’t want to get pregnant – whatever the reason may be,’ Ms Nona said. ‘That’s why they come to see a pharmacist – to ensure the person has the best possible chance of preventing an unintended pregnancy.’
When pharmacists are supported to provide full information and informed choice, patients respond accordingly.
The Australian Pharmaceutical Formulary and Handbook (APF) chapter on ‘Emergency Contraception’, provides essential guidance on:
|

