

 John Jones MPS, pharmacist immuniser and owner of My Community Pharmacy Shortland in Newcastle, NSW[/caption]
John Jones MPS, pharmacist immuniser and owner of My Community Pharmacy Shortland in Newcastle, NSW[/caption]


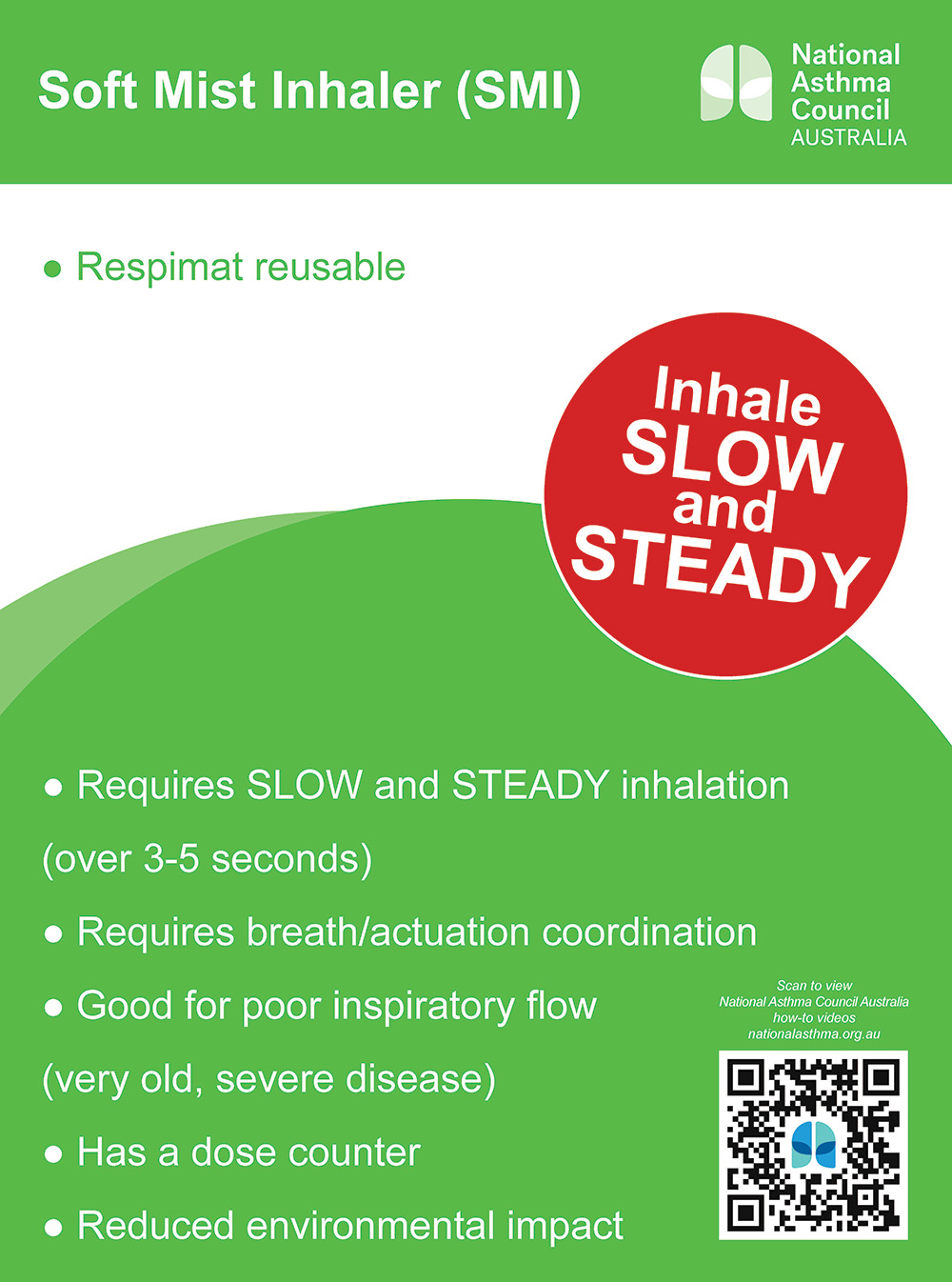
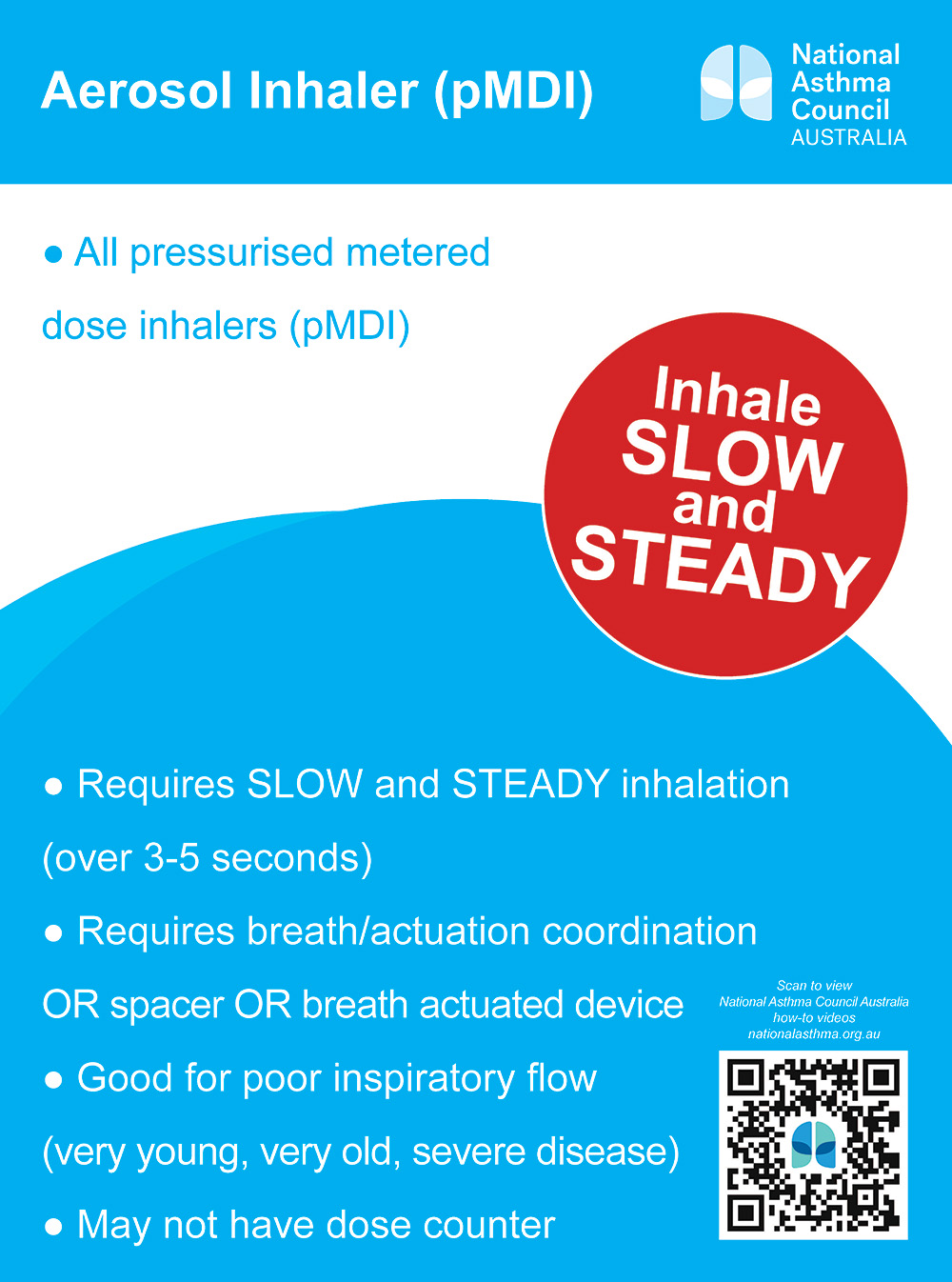
 Debbie Rigby FPS explaining how to correctly use different inhaler devices[/caption]
Debbie Rigby FPS explaining how to correctly use different inhaler devices[/caption]


 Professor Sepehr Shakib[/caption]
Professor Sepehr Shakib[/caption]

 Lee McLennan MPS[/caption]
Lee McLennan MPS[/caption]
 Dr Natalie Soulsby FPS, Adv Prac Pharm[/caption]
Dr Natalie Soulsby FPS, Adv Prac Pharm[/caption]
 Joanne Gross MPS[/caption]
Joanne Gross MPS[/caption]

Case scenario
Lawrence, 66, was diagnosed with chronic lymphocytic leukaemia (CLL) following a routine cholesterol test in 2018. His malignant cell-line count was 5.8 x 109/L, and genetic testing revealed he did not have a p53 gene deletion. He underwent the standard FCR protocol in 2018 and had repeated treatments in 2020.
Lawrence says he feels good and is otherwise well. For their upcoming wedding anniversary, Lawrence and his wife would like to travel interstate to visit their son and new grandchild. The destination requires that visitors are fully vaccinated against COVID-19.
Lawrence is concerned about receiving a COVID-19 vaccination. He is ‘immunocompromised’ and worried about the effect a vaccine will have on his CLL and medications. He asks about vaccine exemptions that may allow him to travel.
Learning objectivesAfter successful completion of this CPD activity, pharmacists should be able to:
Competency standards (2016) addressed: 1.5, 2.2, 2.3, 2.4, 3.1, 3.2, 3.5 |
Already read the CPD in the journal? Scroll to the bottom to SUBMIT ANSWERS.
Introduction
Chronic lymphocytic leukaemia (CLL) is the most common form of leukaemia in Australia.1 It affects developing B lymphocytes – specialised white blood cells that produce antibodies in response to infection or disease. The median age of diagnosis is approximately 70 years and incidence is higher in males.2
The exact cause of CLL is unknown; however, exposure to some chemicals, such as Agent Orange, has been implicated.3 There is a familial association; for those with a first-degree relative with CLL, there is approximately an eightfold increase in developing the disease.4
Pathophysiology
CLL is thought to be preceded by a premalignant proliferative disorder known as monoclonal B-cell lymphocytosis (MBL), which has been observed in 5–10% of the population older than 60 years.5 MBL can progress to CLL at approximately 1–2% per year. MBL may initially arise from antigenic stimulation, gene mutations, epigenetic mutations and cytogenetic abnormalities which may occur at the haematopoietic stem cell stage. Further genetic changes/mutations can result in progression to CLL.6
Clinical presentation
CLL is frequently diagnosed incidentally (i.e. persistent elevated white cell count on blood tests performed for other reasons). Occasionally, patients may present with active disease where B symptoms (e.g. unintentional weight loss, persistent fevers and/or drenching night sweats) will be evident.
CLL may be associated with immune dysfunction manifesting as immunodeficiency (with recurrent infections) and/or autoimmune complications. Autoimmune symptoms can include haemolytic anaemia and thrombocytopenia, caused by the production of autoimmune antibodies against red cells or platelets respectively.
When CLL manifests in the lymph nodes instead of the blood and bone marrow, it is referred to as small lymphocytic lymphoma (SLL). CLL and SLL are considered the same disease with the same in key genetic abnormalities, prognosis and treatment.
Diagnosis
CLL may be suspected based on an abnormal full blood count and blood film: an elevated lymphocyte count (normal range 1.5–4.0 x 109/L) may indicate CLL. Elevated lymphocyte counts can also be caused by infections or reactions to a medicine. Malignant lymphocytes observed in the blood film will usually be small in size, have a mature nucleus, and will be frequently smudged due to fragility.2
Diagnosis is confirmed using flow cytometry, which identifies abnormal proteins expressed on the cell surface. CLL cell lines display the usual B-cell antigens CD19, CD20 and CD23, but also CD5, which is aberrantly expressed and characteristic of the disease.7 Flow cytometry can also quantify the population of cells that exhibits this abnormal pattern of protein expression. A population of greater than 5 x 109/L is required for the diagnosis of CLL; below this threshold is considered MBL.2
Prognosis
Without treatment, the prognosis of CLL is extremely variable; survival ranges from a few years to decades, with a median survival time of approximately 10 years. The Rai and Binet classifications are two clinical staging systems used to differentiate prognostic groups in patients with CLL.8,9 Both systems use an algorithm that considers clinical features (e.g. enlarged lymph nodes and spleen) and blood count measures (low platelets or anaemia) to determine patient prognosis. The Rai classification separates patients into Stage I to III, with varied median survival from 19 to 150 months. The Binet classification ranges from Stage A, where the median survival is comparable to age-matched general population, to
Stage C, where there is a median survival of 24 months.
More recently, the addition of genetic (e.g. TP53 mutation) and biochemical (beta-2 microglobulin) assays allow for improved patient prognostication to further guide management.10
Treatment
There are many classes of medicines for CLL, and the choice of treatment will depend on the stage of the disease, the results of genetic tests, and patient age, health and personal preferences.
Numerous studies have shown that starting active treatment in patients with early asymptomatic disease does not confer an increased survival benefit; a ‘watch and wait’ approach is recommended. Patients are usually monitored 3–6 monthly. Guidelines provide the criteria for treatment initiation: for example, the presence of B symptoms, cytopenias (decreased platelet count or anaemia), and/or accelerated progression (e.g. lymphocyte doubling time, size of lymph nodes).11
A current standard of care for patients who are otherwise well and without significant comorbidities is the combination therapy of fludarabine, cyclophosphamide (two cytotoxic medicines), and the anti-CD20 antibody, rituximab (Rituxan). This treatment regimen, known as FCR, has been shown to induce a clinical response in 90% of patients and improve survival (87% at 3 years) compared to prior standards of therapy.12
In patients who are older than 65 years or have significant comorbidities, obinutuzumab (Gazvya), another anti-CD20 antibody, is used in combination with chlorambucil and has been shown to achieve an overall survival of 91% at 3 years.13
In cases where CLL relapses and has not responded to first-line treatments, other treatments may be considered.
Novel targeted therapy
Cytotoxic therapies have lower efficacy in patients with unfavourable genetic mutations (e.g. TP53 mutation) and in relapsed disease. Novel immune-targeted therapies are used to manage these patients and are increasingly being used in all patient cohorts.
In Australia, the immune-targeted therapies available include ibrutinib, acalabrutinib, venetoclax and idelalisib. Ibrutinib and acalabrutinib are Bruton’s tyrosine kinase (BTK) inhibitors, venetoclax inhibits B-cell lymphoma protein (Bcl-2) and idelalisib inhibits the delta-isoform of phosphatidylinositol 3-kinase (PI3Kδ). Both BTK and PI3K are associated with signalling from the B-cell receptor, ultimately leading to B-cell survival and proliferation. Disruption of these pathways leads to apoptosis of CLL cells. Conversely, Bcl-2 is a protein significantly upregulated in CLL cells, allowing them to evade apoptosis and proliferate. Inhibition of Bcl-2 with venetoclax has been shown to induce rapid CLL cell death.2
Targeted immune-therapies have become standard care in the treatment of relapsed/resistant CLL, especially in those with high-risk mutations. They are increasingly used in the frontline setting, particularly in patients with high risk disease.2
Monitoring
Patients need to be monitored for treatment response and adverse effects. For those in remission, ongoing surveillance for disease relapse is required. Patients receiving chemoimmunotherapy are closely monitored in a specialist setting at the local cancer centre.
Community pharmacists are likely to have a direct encounter with patients’ prescribed targeted therapy as they can be dispensed in community pharmacies.
Ibrutinib (Imbruvica)
Ibrutinib acts by irreversibly binding to BTK proteins. Along with acalabrutinib, it belongs to the class of medicines called BTK inhibitors.
The standard initiation dose is 420 mg orally daily, taken at the same time every day.14 Dose reduction may be required to manage toxicities.
Ibrutinib is a substrate of cytochrome P450 (CYP) enzyme 3A4. Strong inhibitors or inducers should be avoided where possible. If a prolonged course of moderate CYP3A4 inhibitor cannot be avoided, dose reduction may be required.15
Common adverse effects include skin rash, diarrhoea and fatigue. Major haemorrhage occurs in up to 9% of patients, and up to half of patients experience increased bruising.16 Patients should be advised to seek medical attention if there is unusual bruising or bleeding. Co-administration of antiplatelet and anticoagulant medicines further increases bleeding risk and should be avoided where possible. Patients should inform their haematologist when concomitant antiplatelet or anticoagulant therapy has been started.
Cardiac rhythm disorders, in particular atrial fibrillation and flutter, are frequently reported in patients taking ibrutinib. More severe arrhythmias such as ventricular tachycardias have also been described. Other cardiac effects include new or worsening hypertension; regular blood pressure monitoring should be advised.16,17
Acalabrutinib (Calquence)
Acalabrutinib is a second-generation BTK inhibitor with higher specificity to BTK than ibrutinib. Comparative trials have shown that it may be better tolerated than ibrutinib with a lower effective dose and potentially fewer bleeding complications.18 Trials are ongoing, and as such ibrutinib is currently preferred due to weight of evidence.
The standard dose of acalabrutinib is 100 mg orally twice daily. Drugs that increase gastric pH such as proton pump inhibitors should be avoided, and antacids should be separated by 2 hours. Like ibrutinib, it is a substrate of CYP3A4.
Venetoclax (Venclexta)
Venetoclax inhibits Bcl-2, an over-expressed homeostatic protein that helps CLL cells survive longer than they should. It is started at 20 mg daily, increasing to a target dose of 400 mg daily.14 Tablets are taken orally once daily, and should be taken with food at the same time every day. Bioavailability is reduced when taken on an empty stomach.
Gradual dose titration is required to reduce the risk of tumour lysis syndrome, a life-threatening complication where rapid tumour cell death leads to the release of intracellular ions, nucleic acids, protein and metabolites into the systemic circulation. This results in significant electrolyte disturbances and hyperuricaemia, which can lead to renal failure, cardiac arrhythmias, seizures, neurological complications and death.19
Venetoclax is a substrate of the CYP3A4 enzyme. Concurrent administration of inhibitors or inducers of CYP3A4 should be avoided where possible. Strong inhibitors are contraindicated during the dose titration phase. If a moderate or strong CYP3A4 inhibitor must be used, a dose reduction of 50–75% may be required.20
Idelalisib (Zydelig)
Idelalisib inhibits the delta isoform of the phosphoinositide 3-kinase enzyme, also known as P110δ, which is important in regulation of the cell cycle in leukocytes. It is used with rituximab in relapsing CLL where other treatments have not been successful.21 The standard dose of idelalisib is 150 mg orally twice daily.14
It is both a substrate and inhibitor of CYP3A4, therefore coadministration of idelalisib with other CYP3A4 substrates or medicines with narrow therapeutic index should be avoided, where possible.22
Common adverse effects include fever, fatigue, nausea and diarrhoea. Potentially life-threatening adverse effects include hepatic dysfunction, severe diarrhoea/colitis and pneumonitis.23
Regular liver function monitoring is required. Patients with worsening diarrhoea, abdominal pain and nausea should be referred to discuss this with their treating physician. Diarrhoeal illness in some cases may require dose modification. Drug cessation may be required in severe cases of colitis and bowel perforations. Cough, fevers and/or shortness of breath may be symptoms of pneumonia or non-infectious pneumonitis. Patients should be referred for medical attention if these symptoms develop.23
Infection risk
Patients with CLL may be at an increased risk of infection, even prior to the initiation of treatment. Treatment with both cytotoxic and immune-targeted therapies will further increase infection risk, and symptomatic patients (e.g. fever) should be referred to hospital immediately.11
Patients with CLL should have annual influenza as well as pneumococcal vaccinations.24 Vaccine efficacy is decreased after treatment, particularly with B-cell depleting therapies such as rituximab and ibrutinib. Live attenuated vaccines are contraindicated in patients with CLL as death has occurred.25
Knowledge to practice
Counselling patients with CLL who are using oral immune-targeted therapies may follow the approach described previously for chronic myeloid leukaemia (see ‘Chronic myeloid leukaemia’, Australian Pharmacist, October 2020). Pharmacists should explain the mechanism of action, key adverse effects and dosing directions. Drug interactions should also be reviewed, and drug adherence should be encouraged and enabled. Poor drug adherence can potentially impact clinical outcome and increase the risk of disease progression.26
Future directions
Ongoing clinical trials are focused on the optimal sequencing or combination of these therapies. Preliminary results have shown that combinations of cytotoxic and immune-targeted medicines are effective in the eradication of ‘minimal residual disease’ that may lead to durable remission and a prospect of cure.27,28 Future treatments under investigation include whole-cell, antibody, and cytotoxic-free therapies.29
Case scenario continuedLawrence is naturally cautious about his illness and treatment; he is worried that a vaccine will overload his immune system. You reassure him that this is unlikely, and that it is best practice for CLL patients to ensure they are fully vaccinated. On balance, CLL patients are less sick and live longer if they are fully vaccinated. The vaccination will reduce his risk of becoming very ill, and with a dose interval of 4–6 weeks, the sooner he receives his first dose the sooner he will be able to travel. After three rounds of FCR to date, Lawrence asks if you know what the next steps are. You discuss the role of immune-targeted therapies and explain that they treat cancer by a different mechanism and are often useful when the original treatment hasn’t worked. You encourage Lawrence to discuss them with his treating team, which would be best placed to advise for his situation. Lawrence appreciates the advice and seems relieved. |
Conclusion
The management of CLL has changed dramatically in the last decade with the introduction of novel oral immune-targeted therapies. There are increasing opportunities for pharmacists to contribute to the multidisciplinary care of patients with CLL to ensure medicine safety and best patient outcomes.
Key points:
- Chronic lymphocytic leukaemia is the most common form of leukaemia in Australia; incidence increases with age.
- Disease progression is extremely variable; some patients do not require therapy for a decade or more, while others progress rapidly and will require multiple lines of therapy.
- Oral immune-targeted therapies, such as venetoclax, ibrutinib, idelalisib and acalabrutinib, are gradually replacing cytotoxic medicines in many clinical settings.
- Oral immune-targeted therapies are more convenient for patients and require less in-hospital treatment; however, their use is not without potentially serious adverse effects.
This article is accredited for group 2 CPD credits. Click submit answers to complete the quiz and automatically record CPD against your record.
If you do get an enrolment error, please click here![]()
References
- Australian Institute of Health and Welfare. Cancer data in Australia [Internet]. 2015. At: www.aihw.gov.au/reports/cancer/cancer-data-in-australia/contents/summary
- Hallek M. Chronic lymphocytic leukemia: 2020 update on diagnosis, risk stratification and treatment. Am J Hematol 2019 Nov;94(11):1266–87.
- Mescher C, Gilbertson D, Randall NM, et al. The impact of Agent Orange exposure on prognosis and management in patients with chronic lymphocytic leukemia: a National Veteran Affairs Tumor Registry Study. Leuk Lymphoma 2018;59(6):1348–55.
- Slager SL, Caporaso NE, de Sanjose S, et al. Genetic susceptibility to chronic lymphocytic leukemia. Semin Hematol 2013;50(4):296–302.
- Strati P, Shanafelt TD. Monoclonal B-cell lymphocytosis and early-stage chronic lymphocytic leukemia : diagnosis, natural history, and risk stratification. Blood 2019;126(4):454–63.
- Puente XS, Jares P, Campo E. Chronic lymphocytic leukemia and mantle cell lymphoma: crossroads of genetic and microenvironment interactions. Blood 2018;131(21):2–4.
- Rai KR, Sawitsky A, Cronkite EP, et al. Clinical staging of chronic lymphocytic leukemia. Blood 1975;46(2):219–34.
- Binet JL, Auquier A, Dighiero G, et al. A new prognostic classification of chronic lymphocytic leukemia derived from a multivariate survival analysis. Cancer 1981;48(1):198–206.
- An international prognostic index for patients with chronic lymphocytic leukaemia (CLL-IPI): a meta-analysis of individual patient data. Lancet Oncol 2016;17(6):779–90.
- Hallek M, Cheson BD, Catovsky D, et al. iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood 2018;131(25):2745–60.
- Hallek M, Fischer K, Fingerle-Rowson G, et al. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet 2010;376(9747):1164–74.
- Goede V, Fischer K, Busch R, et al. Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N Engl J Med 2014;370(12):1101–10.
- Barr PM, Brown JR, Hillmen P, et al. Impact of ibrutinib dose adherence on therapeutic efficacy in patients with previously treated CLL/SLL. Blood 2017;129(19):2612–5.
- Janssen-Cilag Pty Ltd. Ibrutinib Product Information. 2016.
- Brown JR. How I Treat. How I treat CLL patients with ibrutinib. Blood 2019;131(4):379–87.
- Dickerson T, Wiczer T, Waller A, et al. Hypertension and incident cardiovascular events following ibrutinib initiation. Blood 2019;134(22):1919–28.
- AbbVie Pty Ltd. Venetoclax Product Information. 2020.
- Tambaro FP, Wierda WG. Tumour lysis syndrome in patients with chronic lymphocytic leukaemia treated with BCL-2 inhibitors: risk factors, prophylaxis, and treatment recommendations. Lancet Haematol 2020;7(2):e168–76.
- Gilead Sciences Pty Ltd. Zydelig Product Information. 2017.
- Cuneo A, Barosi G, Danesi R, et al. Management of adverse events associated with idelalisib treatment in chronic lymphocytic leukemia and follicular lymphoma: a multidisciplinary position paper. Hematol Oncol 2019;37(1):3–14.
- Mikulska M, Cesaro S, de Lavallade H, et al. Vaccination of patients with haematological malignancies who did not have transplantations: guidelines from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis 2019;19(6):e188–99.
- Jain N, Keating M, Thompson P, et al. Ibrutinib and venetoclax for first-line treatment of CLL. N Engl J Med 2019;380(22):2095–103.
- Rogers KA, Huang Y, Stark A, et al. Initial Results of the Phase 2 treatment naive cohort in a Phase 1b/2 Study of obinutuzumab, ibrutinib, and venetoclax in Chronic Lymphocytic Leukemia. Blood [Internet] 2017;130(Supplement 1):431. At: https://doi.org/10.1182/blood.V130.Suppl_1.431.431
- Rossi S, ed. Australian medicines handbook. Adelaide: Australian Medicines Handbook; 2020.
- Byrd J, Harrington B, O’Brien S, et.al. Acalabrutinib (ACP-196) in relapsed chronic Lymphocytic leukemia. N Engl J Med 2016;374(4):323–32.
- Furman R, Sharman J, Coutre SE, et al. Idelalisib and rituximab in relapsed chronic lymphocytic leukemia. N Engl J Med 2014; 370:997–1007.
- Hobson R. Vaccinations recommended for patients with chronic lymphocytic leukaemia (CLL) and monoclonal B-cell lymphocytosis (MBL). Harrogate and District NHS Foundation Trust. April 2018. At. www.hdft.nhs.uk/content/uploads/2015/12/Immunisation-in-CLL-updated-branding.docx
- Patel K, Pagel JM. Current and future treatment strategies in chronic lymphocytic leukemia. J Hematol Oncol 2021;14(69). Epub 2021 Apr 26.
- Jaseb k, Purrahman D, Shahrabi S, et.al. Prognostic significance of aberrant CD5 expression in B-cell leukemia. Oncol Rev 2019;13(1):400.
DR ERIC WENLONG LI BPharm(Hons), MBBSis an Advanced Trainee in Haematology at Concord Repatriation General Hospital. He also lectures at the School of Pharmacy at the University of Sydney on topics relating to haematology.




