")









Did you know a new Australian Cardiovascular risk calculator (AusCVDRisk) was released last year?
If not, you’re not alone, said Karl Winckel, pharmacist at Princess Alexandra Hospital and the University of Queensland’s School of Pharmacy.

‘It’s gone under the radar,’ he said. ‘Education about the new tool is mostly targeted at GPs rather than nurses or pharmacists.’
As it turns out, CVD risk has been ‘massively overestimated’ through use of previous CVD risk tables.
With landmark studies such as ASPREE, ARRIVE, ASCEND all showing much lower benefit than expected for aspirin in primary prevention, it’s time to shift approach to preventative care.
To kick off Heart Week (6–12 May 2024), Australian Pharmacist explains how to best wield the new tool to your patients’ advantage.
What was wrong with the previous CVD calculator
Previous CVD risk assessments were based on the ongoing Framingham Heart Study, conducted in the small Massachusetts town of Framingham, dating back to the late 1940s.
But cardiovascular risk has changed significantly since then, with people more aware of the risks, said Mr Winckel.
‘People are also exercising more and using preventative therapies,’ he said.
The new AusCVDRisk tool uses QRISK3 risk prediction model and PREDICT model incorporating data from the United Kingdom and New Zealand, with baseline risk adjusted to suit the Australian context.
‘They looked at all the Australian Bureau of Statistics (ABS) and relevant surveys in New Zealand to dictate the number of strokes and heart attacks in different age and comorbidity brackets,’ he said.
There was also lack of nuance when using the Framingham risk tables. For example, when users classified their smoking habits, they would simply click ‘smoker’ or ‘non-smoker’.
‘That means if you quit smoking a week ago, that classifies you as a nonsmoker, but you might have been smoking for 30 years,’ Mr Winckel said.
While CVD risk reduces upon cessation, it never returns to baseline. With AusCVDRisk, users can include more details about their smoking history, including if they’re a never-smoker or ex-smoker.
To demonstrate the variation in risk estimation between the Framingham and AusCVDRisk tools, the author calculated a family member’s CVD risk using both. The former placed their risk at 5–10% over 5 years. Using AusCVDRisk, it was 2%.
What are the benefits of the new calculator?
When it comes to calculating CVD risk, the devil is in the details.
More information is included in AusCVDRisk about users’ diabetes history to quantify a more accurate risk score, including:
- HbA1c levels
- insulin use.
‘If you have type 2 diabetes and use insulin, your diabetes is likely to be more poorly controlled, so you’d likely have more vascular system damage,’ he said.
But one of the most important factors included in the new calculator is Socio-Economic Indexes for Areas quintiles obtained from postcodes as a measure of socioeconomic status, which can even detect variation in risk within the same city. Within the quintile ranking system, 1 being the most disadvantaged postcode and 5 being the most advantaged, those in the lowest ranked suburbs had more incidents of strokes and heart attacks, according to ABS statistics.
‘Socioeconomic status is the biggest risk to CV health, more than smoking,’ Mr Winckel said. ‘The best estimate of impact of socioeconomic status on health is residence, as shown in many studies both locally, and in the UK in places such as Scotland.’
How can pharmacists best use the tool?
Pharmacists, particularly those who practise in lower socioeconomic areas, can use the tool during health campaigns to raise awareness about CVD risk.
‘Once you’ve calculated the estimate, you can print off pictures to see your comparative risk,’ said Mr Winckel.
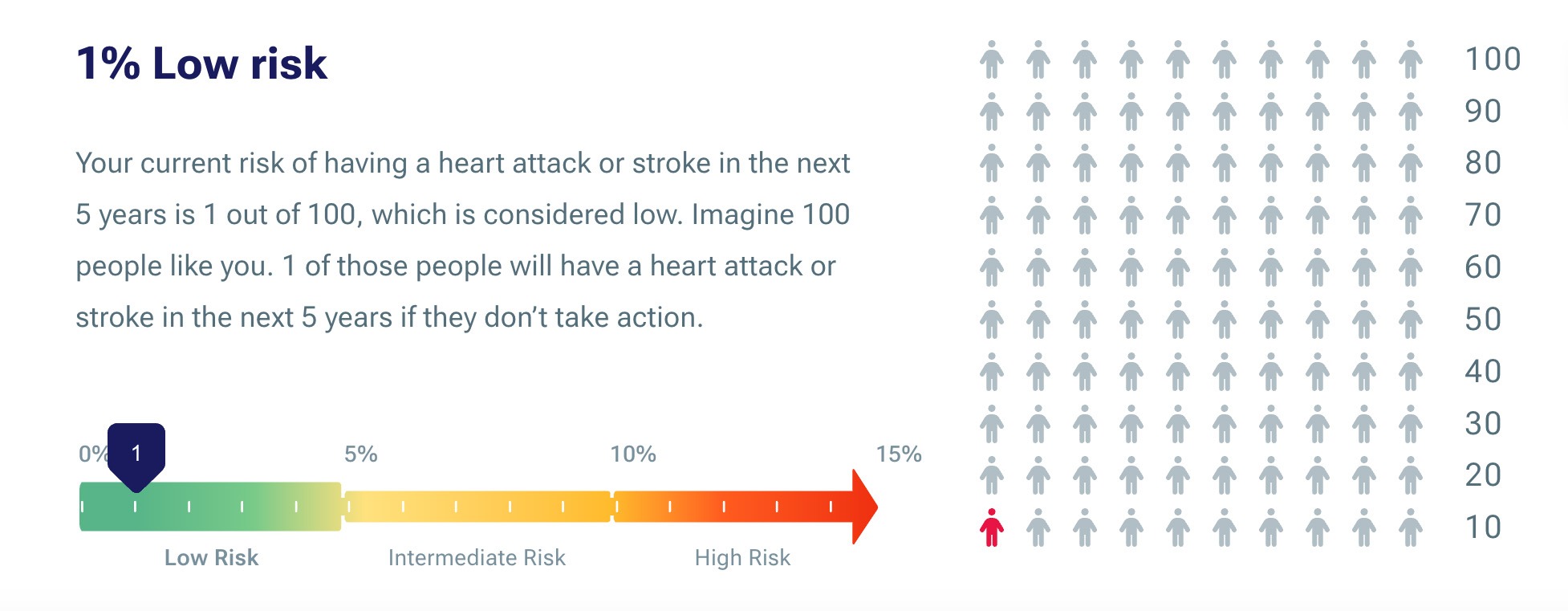
Patients can also determine their risk once they hit certain health goals, including:
- lowering LDL one millimoles per litre (mmol/L)
- reducing blood pressure by 10 mm of mercury (mmHg).
‘Those numbers are smartly linked, because that’s what you might expect by complying to a first antihypertensive or moderate dose of a statin,’ he said.
AusCVDRisk could also be used to preface discussions about the importance of smoking cessation by quantifying the CVD risks associated with smoking.
‘Using the calculator, you could show the impact of lowering LDL by one millimoles per litre or changing smoking [status], and say “quitting smoking is more impactful than anything else”,’ he said.
Coupling this approach with the Heart Foundation’s ‘Cost of smoking’ calculator could help to hit the message home.
What about aspirin?
When the Framingham calculator was used, the common approach was to recommend low-dose aspirin (LDA) to anyone whose CV risk was over 10%. With LDA purported to reduce cardiovascular events by around 20% and carry less than 1% risk of gastro-intestinal (GI) bleeding, which was dispelled by the aforementioned studies, this was the go-to approach, said Mr Winckel.
“Effectively, that meant if you were over 40, with pretty normal blood pressure and LDL levels, you could have been recommended LDA,’ he said.
Now, plenty of patients in their 50s and 60s who have been on aspirin for lengthy periods of time due to an overestimation of baseline risk are likely to have benefitted little from this approach, said Mr Winckel.
‘The reduction in their baseline risk from aspirin is less in terms of a percentage.’
Bleeding risk from LDA was also underestimated, particularly for older demographics.
‘We now know if you’re over 60, your GI and major bleeding risk with aspirin is much higher, and sometimes increases by 2%.’
With its dual effect of antiplatelet effect and erosion of GI mucosa, aspirin poses a greater bleeding risk than drugs such as clopidogrel, Mr Winckel thinks.
‘We’re primed to think aspirin is a low-risk drug because it’s available over-the-counter, but dual antiplatelets significantly increase bleeding risk.’
What should pharmacists look out for?
Pharmacists should detect unnecessary and/or harmful uses of primary prevention, based on updated CVD risk, at any opportunity they have to review or consider a patient’s medicine profile.
This should be a key consideration for credentialed pharmacists conducting Home Medicines Reviews or Residential Medication Management Reviews.
Aside from antiplatelets, antihypertensives (which can lead to a significant drop in blood pressure among older patients) should also be investigated, along with beta blockers for primary hypertension, said Mr Winckel.
‘Beta blockers generally increase mortality for many frail elderly people by increasing risk of falls and subsequent fractures,’ he said. ‘When patients are not currently hypertensive, all hypertensives should be reviewed.’
But cessation of antiplatelets should only be considered when used in primary prevention, Mr Winckel warned. ‘If used for secondary prevention, lifelong antiplatelet therapy is required.’


