

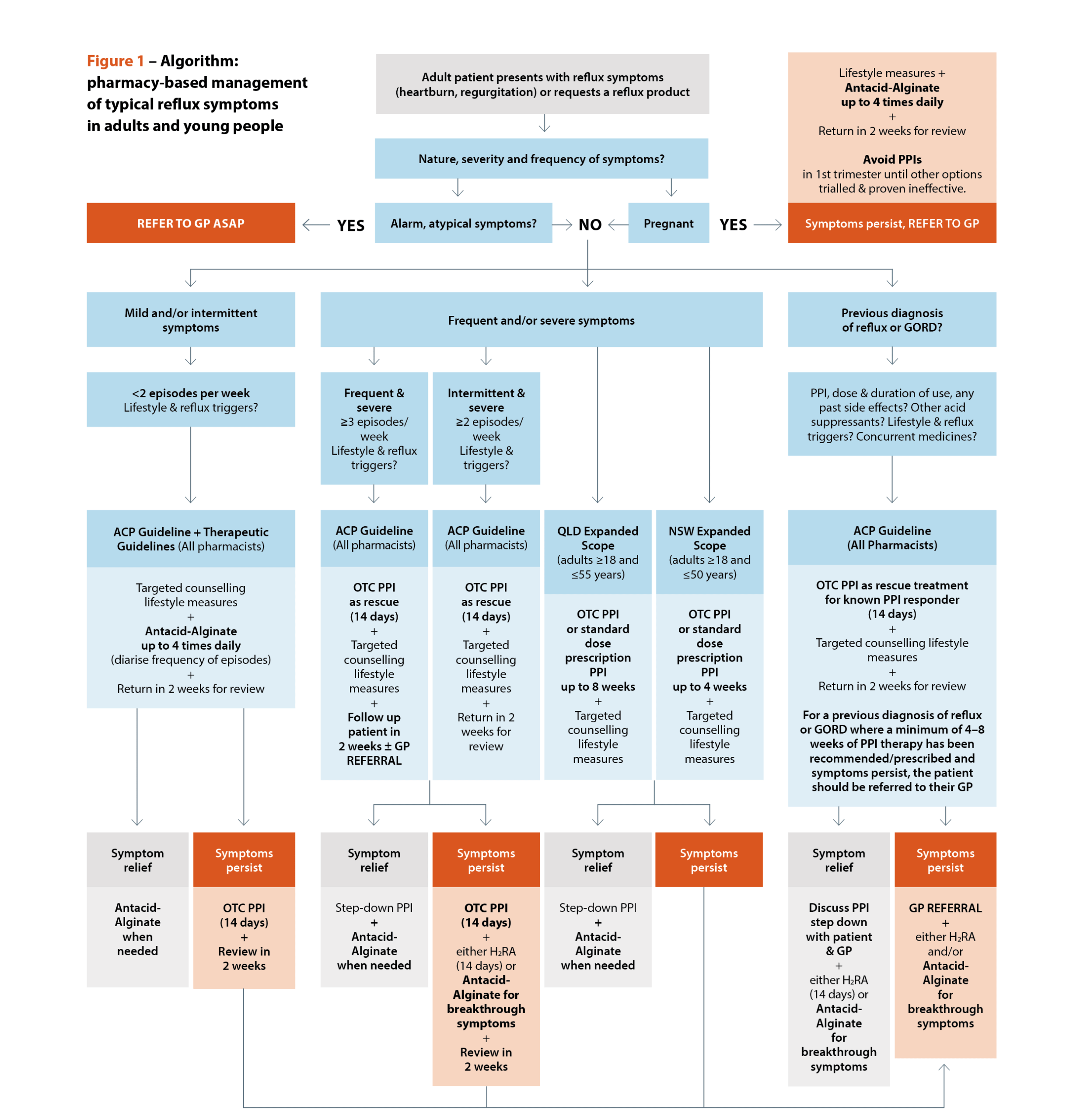
 Sources: Australasian College of Pharmacy. Management of reflux: a guideline for pharmacists. Queensland Health. Queensland Community Pharmacy Gastro-oesophageal Reflux and Gastro-oesophageal Reflux Disease – Clinical Practice Guideline. NSW Health. NSW Pharmacist Practice Standards for gastro-oesophageal reflux and gastro-oesophageal reflux disease.[/caption]
Sources: Australasian College of Pharmacy. Management of reflux: a guideline for pharmacists. Queensland Health. Queensland Community Pharmacy Gastro-oesophageal Reflux and Gastro-oesophageal Reflux Disease – Clinical Practice Guideline. NSW Health. NSW Pharmacist Practice Standards for gastro-oesophageal reflux and gastro-oesophageal reflux disease.[/caption]

 Dr Ming S Soh PhD, BPharm (Hons)[/caption]
Dr Ming S Soh PhD, BPharm (Hons)[/caption]





 DR Amy Page (she/her) PhD, MClinPharm, GradDipBiostat, GCertHProfEd, GAICD, GStat, FSHPA, FPS is a consultant pharmacist, biostatistician, and the director of the Centre for Optimisation of Medicines at UWA’s School of Allied Health.[/caption]
DR Amy Page (she/her) PhD, MClinPharm, GradDipBiostat, GCertHProfEd, GAICD, GStat, FSHPA, FPS is a consultant pharmacist, biostatistician, and the director of the Centre for Optimisation of Medicines at UWA’s School of Allied Health.[/caption]

 Hui Wen Quek (she/her) BPharm(Hons), GradCertAppPharmPrac is a pharmacist and PhD candidate at the University of Western Australia (UWA).[/caption]
Hui Wen Quek (she/her) BPharm(Hons), GradCertAppPharmPrac is a pharmacist and PhD candidate at the University of Western Australia (UWA).[/caption]

 Gauri Godbole FPS[/caption]
Gauri Godbole FPS[/caption]

A recent report conducted by the Coroners Court of Victoria found that overdose deaths in 2024 were the highest they have been in a decade.
And of the 584 Victorians who died of an overdose last year, a stark proportion were related to illegal drugs, said Associate Professor Shalini Arunogiri, NHMRC Emerging Leader Research Fellow at Monash Addiction Research Centre and Eastern Health Clinical School.
‘A decade ago, they accounted for less than 50% of overdose deaths. But in 2024, that contribution is now 65% – with a year-on-year increase in the last few years.’
A significant contributor to this trend is the increase in heroin-related deaths, with 248 deaths in the last year compared to 204 in 2023.
‘There has also been a significant increase in the number of methamphetamine-related deaths – which have tripled over the last decade [to 215 deaths],’ A/Prof Arunogiri said.
A sub-analysis of the report, looking at accidental versus intentional overdose, found the vast majority (75%) of deaths were accidental. Men aged 35–54 were also most at risk, as are those who live in urban areas – with three-quarters of deaths occurring in metropolitan Melbourne.
‘[But] in the cases where it was thought to be intentional, women are over-represented in that group,’ she said.
What’s driving these trends?
A good indicator is understanding who’s accessing treatment, A/Prof Arunogiri said.
‘We have treatment-specific data that we can compare and contrast with, and then we also have national survey data,’ she said.
‘From both those sources, what we see is a high proportion of the opioid-related [treatment] cases are prescription opioids’.
In other words, those accessing opioid replacement therapy (ORT) are more likely to be patients who use prescription, rather than illegal, opioids – leaving the latter more susceptible to overdose.
‘We’ve seen extended waits for people to access prescribing and treatment in the Victorian setting,’ she said. ‘It’s a concerning trend to see a rise in heroin-related deaths because people are not able to get into treatment quickly for opioids at the moment.’
Another potential contributor to overdose deaths linked to illegal drugs is contaminants in the supply – including novel synthetic opioids such as nitazenes. However, we won’t know the impact of this straight away, A/Prof Arunogiri said.
‘This is a very quickly emerging trend,’ she said. ‘With the most recent data on [this] report being the full year of 2024, it might not reflect exactly what we’re seeing on the ground just yet. But we’d be expecting that in the next year of data there will be a potential escalation in those deaths.’
What role is prescribing playing?
Since 2020, there has been a downturn in the number of overdose deaths related to pharmaceutical opioids.
This could be because opioid prescribing in Australia decreased by 21% between 2015 and 2022, driven by a series of regulatory and policy changes. This includes the tightening of prescribing rules in June 2020, which set limits on repeat scripts, mandated smaller pack sizes for immediate-release opioids and increased requirements for prescriber authorisation.
However, Australia still ranks among the top countries in per-capita opioid prescribing, with opioids remaining the primary cause of drug-induced deaths. And Victoria’s real-time prescription monitoring system, SafeScript, doesn’t appear to be reducing high-risk opioid prescribing.
A 2023 study found that there was no significant impact on the prescribing of high-dose opioids or high‑risk combinations such as opioids with benzodiazepines or pregabalin. Instead, reductions occurred in low‑dose opioid prescribing. And at the same time, there was evidence of unintended substitution effects, with increased initiation of medicines such as tricyclic antidepressants, pregabalin and tramadol.
While not a major contributor to annual overdose deaths, the number of pregabalin-related deaths have risen – reaching 92 in 2024, versus 34 in 2015.
With gabapentinoids (pregabalin and gabapentin) and tramadol added to SafeScript 2 years ago, A/Prof Arunogiri said it will be interesting to see what occurs in this space.
‘We particularly want to keep an eye on pregabalin-related deaths,’ she said.
What are the bottlenecks to ORT access?
Reforms to Pharmaceutical Benefits Scheme (PBS) Opioid Dependence Treatment (ODT) medicine arrangements have widened access to treatment by improving affordability.
But in Victoria, the vast majority of ORT prescribing occurs within general practice settings rather than public sector settings, A/Prof Arunogiri said.
‘So the block, rather than being a dispensing issue, is on the prescribing end – with the waits to get into treatment increasing over time,’ she said.
‘When prescribers retire, there’s a huge bottleneck preventing people from getting into treatment, because it’s such a small prescribing pool in the state.’
Within Victoria, there’s been significant advocacy for systemic reform of the opioid pharmacotherapy system to reduce wait times and increase public sector involvement.
Shared-care involvement in ORT programs should help to improve access and engagement with therapy.
‘There are novel pharmacy shared care models that are starting to be trialled,’ A/Prof Arunogiri said.
‘This supports pharmacists’ involvement, not just at the dispensing end, but also in prescribing – including working with local GPs in a model that enables expanded access to medication.’
Across the country, the message appears to be getting through about ODT for people who are dependent on prescription opioids.
‘This is a growing proportion of our population. In some settings, more than 50% of our client group is prescription opioid dependent,’ she said.
What else needs to change?
An engagement and expansion of Take Home Naloxone (THN) programs – not just in Victoria, but nationally.
Within Victoria, an investment in expanding access to THN is already occurring.
‘We’re looking at a trial of vending machines to be able to dispense THN,’ A/Prof Arunogiri said.
Located at health services such as community health centres and hospitals in Melbourne’s central business district and inner suburbs, the vending machines are proposed to provide free naloxone and must maintain medicine stability.
‘If pharmacists can be engaged in that process, and promote and advertise awareness of THN – that will be a huge help in preventing these overdoses,’ she said.
Where possible, pharmacies should stock both intranasal and injectable THN formulations.
‘This can help to demystify the process for the lay public, who may be less comfortable administering an injectable product,’ she A/Prof Arunogiri said.
Promoting understanding that naloxone is a safe substance that’s life-saving when administered to someone experiencing an overdose, is also key.
‘We’re also really advocating for awareness of THN for people who are prescribed opioids,’ A/Prof Arunogiri said. ‘If you’re prescribed an opioid analgesic, you should have access to THN – that’s anyone who has hip or back pain, or is prescribed strong opioids for these types of indications.’
Some people have raised concerns about giving naloxone to an unconscious person who may not be experiencing an opioid overdose.
‘But there’s no risk; naloxone also won’t interact with anything aside from opioids,’ A/Prof Arunogiri said.
To enhance clinical outcomes and medication safety for people using prescription opioids for chronic pain, access the Opioid Safety Toolkit – co-developed by PSA, Monash University and PainAustralia – which includes an opioid safety plan template, consumer-facing posters and Routine Opioid Outcomes Monitoring templates.


