



 A national education program for pharmacists funded by the Australian Government under the Quality Use of Diagnostics, Therapeutics and Pathology program.[/caption]
A national education program for pharmacists funded by the Australian Government under the Quality Use of Diagnostics, Therapeutics and Pathology program.[/caption]
 The hypothalamus houses neurons that produce neuropeptides called orexin A and B, which were discovered in 1998, and represent one of the most exciting discoveries in sleep medicine.5,13–15 Orexin-producing neurons help us stay awake and alert, especially when we really need to focus, which is critical for survival.5,14 These neurons reach out to many brain areas that use other wakefulness messengers such as acetylcholine, dopamine, histamine, serotonin and noradrenaline. These areas ‘talk back’ to the hypothalamus, to further boost wakefulness signals.5 Similarly, the thalamus is an important region that also serves to relay wakefulness signals from the RAS.5
The hypothalamus houses neurons that produce neuropeptides called orexin A and B, which were discovered in 1998, and represent one of the most exciting discoveries in sleep medicine.5,13–15 Orexin-producing neurons help us stay awake and alert, especially when we really need to focus, which is critical for survival.5,14 These neurons reach out to many brain areas that use other wakefulness messengers such as acetylcholine, dopamine, histamine, serotonin and noradrenaline. These areas ‘talk back’ to the hypothalamus, to further boost wakefulness signals.5 Similarly, the thalamus is an important region that also serves to relay wakefulness signals from the RAS.5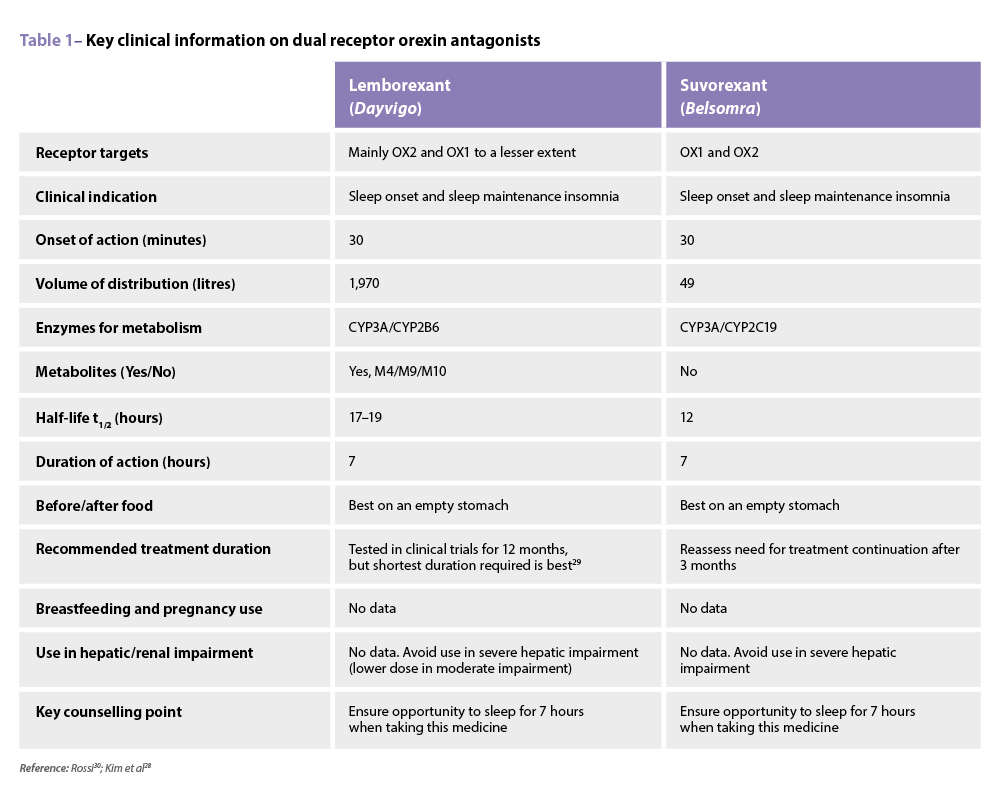 Another dual orexin receptor antagonist (DORA), vornorexant*, is under development and currently undergoing clinical trials.28
Another dual orexin receptor antagonist (DORA), vornorexant*, is under development and currently undergoing clinical trials.28  Other medicines such as dimdazenil* (partial positive allosteric modulator at GABAA specific to alpha-1 and alpha-5 GABAA receptor subtypes)41 and zuranolone* (positive allosteric modulator for GABAA) have also been tested, with positive outcomes in trials. Zuranolone* is marketed overseas specifically for postnatal depression, but clinical trials for its use in insomnia are ongoing.40
Other medicines such as dimdazenil* (partial positive allosteric modulator at GABAA specific to alpha-1 and alpha-5 GABAA receptor subtypes)41 and zuranolone* (positive allosteric modulator for GABAA) have also been tested, with positive outcomes in trials. Zuranolone* is marketed overseas specifically for postnatal depression, but clinical trials for its use in insomnia are ongoing.40

 Kristy Carter (she/her)
Kristy Carter (she/her)
 Louise Edwards (she/her)
Louise Edwards (she/her) 

In introducing the new medicinal cannabis regulatory framework last year, the Government’s intent was to provide patient access to Australian-grown and manufactured medicinal cannabis products, initially outside the standard registered medicines route.
Australia differs from countries such as the...

Pharmacists are embracing new opportunities to play a greater role in multidisciplinary teams focused on mental health.
Australian Pharmacist spoke with two mental health experts – one a practising pharmacist and the other a former general practitioner (GP) –...

The emerging role for Australian pharmacists working in general practices is seen by many pharmacists as an exciting new career opportunity.
It is supported and promoted by the Pharmaceutical Society of Australia, the Australian Medical Association and the Royal...

The legalisation and supply of medicinal cannabis in Australia and elsewhere is making rapid strides despite a relative lack of evidence for its benefits.
With the Federal Government easing supply and Victoria harvesting the nation’s first legal crop of...

