


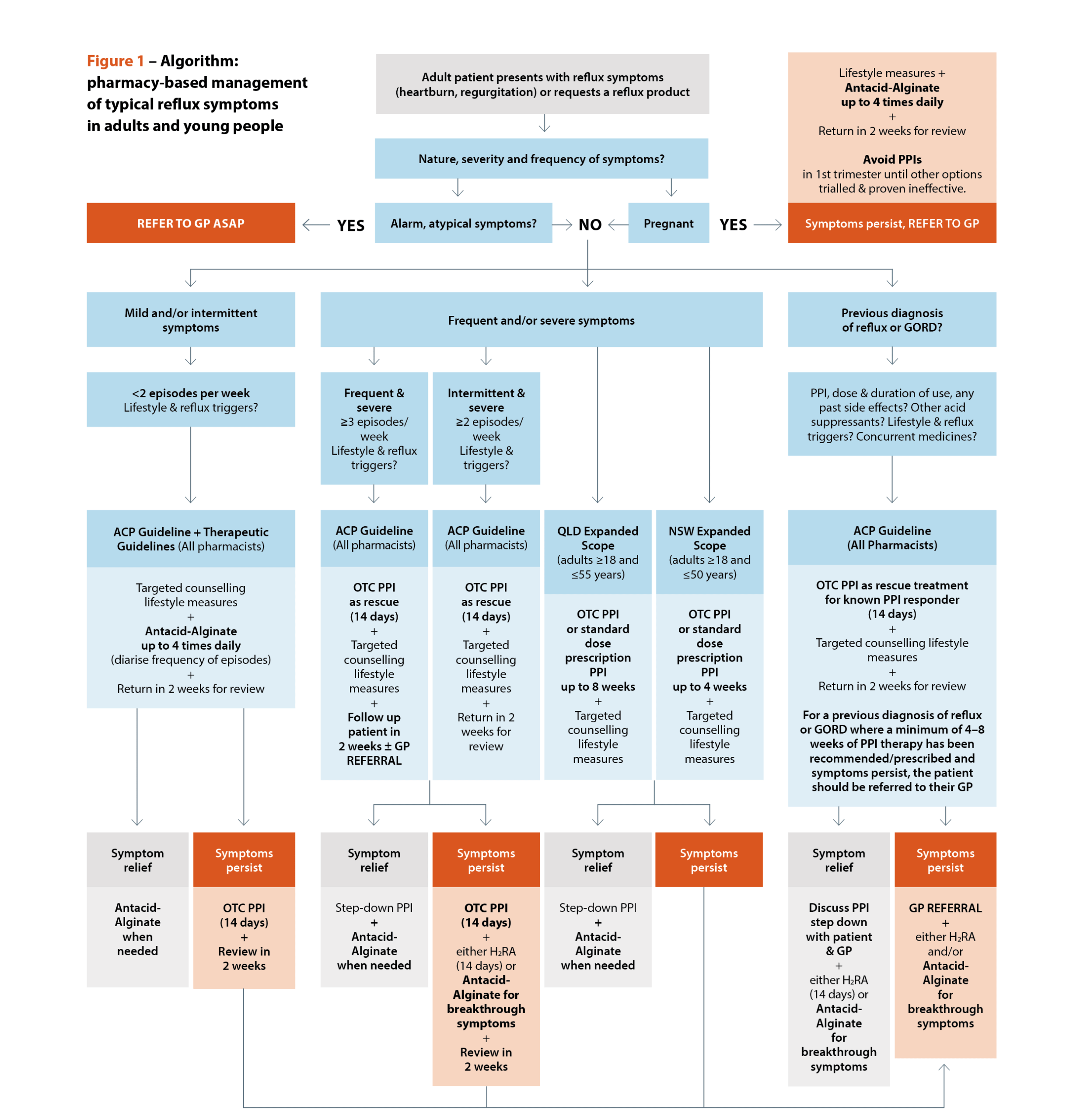
 Sources: Australasian College of Pharmacy. Management of reflux: a guideline for pharmacists. Queensland Health. Queensland Community Pharmacy Gastro-oesophageal Reflux and Gastro-oesophageal Reflux Disease – Clinical Practice Guideline. NSW Health. NSW Pharmacist Practice Standards for gastro-oesophageal reflux and gastro-oesophageal reflux disease.[/caption]
Sources: Australasian College of Pharmacy. Management of reflux: a guideline for pharmacists. Queensland Health. Queensland Community Pharmacy Gastro-oesophageal Reflux and Gastro-oesophageal Reflux Disease – Clinical Practice Guideline. NSW Health. NSW Pharmacist Practice Standards for gastro-oesophageal reflux and gastro-oesophageal reflux disease.[/caption]

 Dr Ming S Soh PhD, BPharm (Hons)[/caption]
Dr Ming S Soh PhD, BPharm (Hons)[/caption]





 DR Amy Page (she/her) PhD, MClinPharm, GradDipBiostat, GCertHProfEd, GAICD, GStat, FSHPA, FPS is a consultant pharmacist, biostatistician, and the director of the Centre for Optimisation of Medicines at UWA’s School of Allied Health.[/caption]
DR Amy Page (she/her) PhD, MClinPharm, GradDipBiostat, GCertHProfEd, GAICD, GStat, FSHPA, FPS is a consultant pharmacist, biostatistician, and the director of the Centre for Optimisation of Medicines at UWA’s School of Allied Health.[/caption]

 Hui Wen Quek (she/her) BPharm(Hons), GradCertAppPharmPrac is a pharmacist and PhD candidate at the University of Western Australia (UWA).[/caption]
Hui Wen Quek (she/her) BPharm(Hons), GradCertAppPharmPrac is a pharmacist and PhD candidate at the University of Western Australia (UWA).[/caption]

Case scenario
Mrs Patel, a 58-year-old female with poorly controlled type 2 diabetes mellitus (T2DM) and hypertension, visits you requesting a blood pressure check. You learn that she has been experiencing fatigue and leg swelling and has not had recent blood tests. She is taking metformin 850 mg three times daily, perindopril 5 mg each morning, and over-the-counter herbal supplements. You recognise that Mrs Patel has multiple CKD risk factors.
Learning objectivesAfter reading this article, pharmacists should be able to:
Competency standards (2016) addressed: 1.1, 1.4, 1.5, 2.2, 3.1, 3.5 Accreditation number: CAP2511CDMRC Accreditation expiry: 31/10/2028 |
Already read the CPD in the journal? Scroll to the bottom to SUBMIT ANSWERS.
Introduction
Chronic kidney disease (CKD) is a progressive long-term condition characterised by a gradual and usually irreversible decline in kidney function.1 It is defined as a sustained reduction (for 3 months or more) in the measured or estimated glomerular filtration rate (eGFR) to <60 mL/min/1.73 m2 with or without evidence of kidney damage OR evidence of kidney damage (e.g. albuminuria, haematuria) for 3 months or more with or without reduced eGFR.1,2 Due to these changes, CKD is associated with adverse clinical outcomes including end-stage kidney disease (ESKD), cardiovascular disease (CVD), hypertension, stroke and increased mortality.1,2
THIS IS A CPD ARTICLE. YOU NEED TO BE A PSA MEMBER AND LOGGED IN TO READ MORE.
