


 Ruth Nona[/caption]
Ruth Nona[/caption]

 Kate Gunthorpe MPS[/caption]
Kate Gunthorpe MPS[/caption]
 Madison Low[/caption]
Madison Low[/caption]


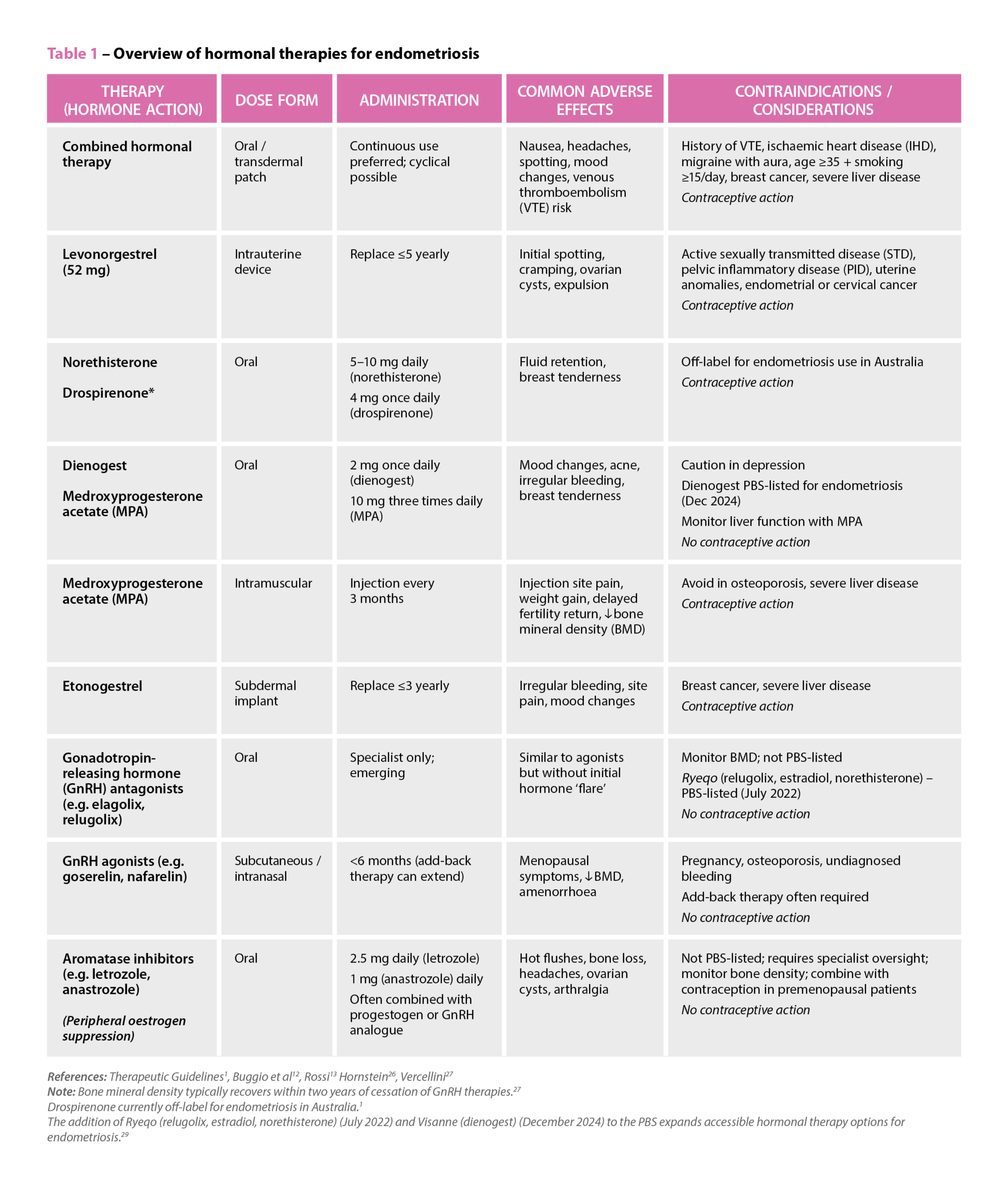 References: Therapeutic Guidelines
References: Therapeutic Guidelines
In a significant advancement for patient-centred care, a team of pharmacists from the University of Tasmania is reshaping the landscape of antidepressant deprescribing.
Their latest research aims to close a long-standing clinical gap by making easy-to-prepare, cost-effective oral liquid formulations of commonly prescribed antidepressants accessible to every Australian pharmacist.

These new formulas will help to ensure that patients have options to access safe and effective medications when deprescribing antidepressants, said Natalie Cooper, Research Project Lead at the University of Tasmania’s School of Pharmacy and Pharmacology.
‘Prescribers can also have confidence that when they are prescribing these formulas and suggesting a deprescribing regime, the patient is going to receive an accurate and effective dose,’ she said.
Long-term use with limited tapering options
Each year, over 3.5 million Australians are prescribed antidepressants. Half of these patients become long-term users, with average treatment durations reaching 4 years – well beyond the recommended 6–12 month course to treat a single depressive episode. While these medicines play a critical role in managing mental health, extended use can result in adverse effects, particularly in older adults. Yet safely discontinuing antidepressants remains a challenge.
Key among the hurdles is dose inflexibility.
‘With the lack of commercially available liquid antidepressant formulations available in Australia, there are limited dosing options for people to withdraw from antidepressant medications,’ Ms Cooper said.
The recently released Maudsley Deprescribing Guidelines recommend a hyperbolic tapering method – small, incremental decreases in dose over time – to minimise withdrawal symptoms and support the body’s physiological adjustment. However, this method often requires doses lower than commercially available tablet strengths.
In Australia, the lowest available strength of citalopram – the most commonly prescribed antidepressant – is a 10 mg tablet, which can make safe and effective tapering difficult.
Seeking safer deprescribing methods
When tapering antidepressants, current guidelines often suggest that low doses of certain formulations can be crushed up and dispersed in water, Ms Cooper said.
‘Getting patients to do this imprecise method at home didn’t sound safe to me,’ she said. ‘So I reached out to the Wilson Foundation and asked “why don’t we utilise liquid formulations to [deprescribe] in a safe and effective way?’”
In response, the Wilson Foundation funded an 18-month project aimed at producing professional, evidence-based formulation alternatives that all registered pharmacists can readily compound.
‘By creating easy-to-prepare, cost-effective liquid antidepressant formulations that any pharmacy can compound, we’re tackling a major barrier to antidepressant discontinuation,’ Ms Cooper said.
Choosing the right antidepressants for compounding
The research team selected 11 antidepressants for development, targeting those most commonly prescribed in Australia, including mirtazapine, paroxetine and fluoxetine.
‘There are some that aren’t as commonly prescribed, but if there’s a patient who needs to come off them, they have an option available,’ Ms Cooper said.
Out of 15 antidepressants listed in the Maudsley Deprescribing Guidelines, four were identified as controlled-release formulations – such as venlafaxine – that can’t be easily transformed into liquid forms.
‘We have gone with the antidepressants we know are immediate release and can be formulated into liquid formulations,’ she said.
The formulations that have sustained-release properties will still require a compounding pharmacist’s expertise to formulate alternate dosage forms.
Developing evidence-based liquid formulations
Designed for ease and accessibility, the proposed liquid formulations can be compounded using standard equipment and readily available ingredients.
‘We’re conducting stability testing on these liquid formulations using the commercially available tablets and accessible bases such as ORA-Sweet and ORA-Plus,’ Ms Cooper said. ‘So pharmacists can compound them when they get a prescription from a GP for individual patient supply.’
Once stability and microbial safety are confirmed, the formulations will be submitted to the Australian Pharmaceutical Formulary and Handbook (APF) to be considered for inclusion.
If they are in the APF, they will be available to every single pharmacist and pharmacy in Australia to compound.
The rollout will be incremental, with three formulations submitted each quarter until all 11 are included by the project’s completion.
Bridging gaps in access and affordability
Compounded formulations of antidepressants have traditionally only been available through specialised pharmacies. For patients and prescribers alike, this has presented a barrier to optimal care.
‘Some people may be getting specialised compounded fluoxetine capsules in a low dose through a compounding pharmacy, for example. But they can be quite expensive,’ Ms Cooper said. ‘Accessing a compounding pharmacy also can be quite difficult.’
Dr Anna Seth, a Tasmanian GP, echoed these concerns from the prescriber’s perspective.
‘Existing options for gradual discontinuation of antidepressants are very limited, creating a barrier for patients and the doctors who support them,’ she said. ‘The cost of compounding these medications is prohibitive for many of my patients who are then stuck with either trying to crush and disperse tablets at home or stopping medications more abruptly and risking unpleasant withdrawal effects.’
The new liquid formulations will allow prescribers to instruct patients in volume-based dosing, simplifying the regimen.
Pharmacists’ role in interdisciplinary care
Beyond compounding, pharmacists will play a crucial role in patient and prescriber education.
‘It’s important to get it out through networks to let prescribers know that these formulas are available for pharmacists to compound,’ Ms Cooper said. ‘Communication between the doctor and the pharmacist will help patients be able to achieve effective withdrawal from antidepressants.’
Joanne Gross, President of PSA’s Tasmania Branch, reinforced the importance of pharmacist leadership in deprescribing initiatives.
‘Antidepressant deprescribing remains a challenge, particularly for long-term users experiencing withdrawal symptoms,’ she said.
‘PSA looks forward to continuing to work with the University to potentially make their findings accessible to all Australian pharmacists through the APF, supporting flexible, individualised tapering regimens and improving patient outcomes.’
To find out more about when and how pharmacists can compound and the compliance obligations required, attend the ‘Compounding essentials for 2025’ session at PSA25 held in Sydney from 1–3 August. Register here to attend.

