

 Ruth Nona[/caption]
Ruth Nona[/caption]

 Kate Gunthorpe MPS[/caption]
Kate Gunthorpe MPS[/caption]
 Madison Low[/caption]
Madison Low[/caption]

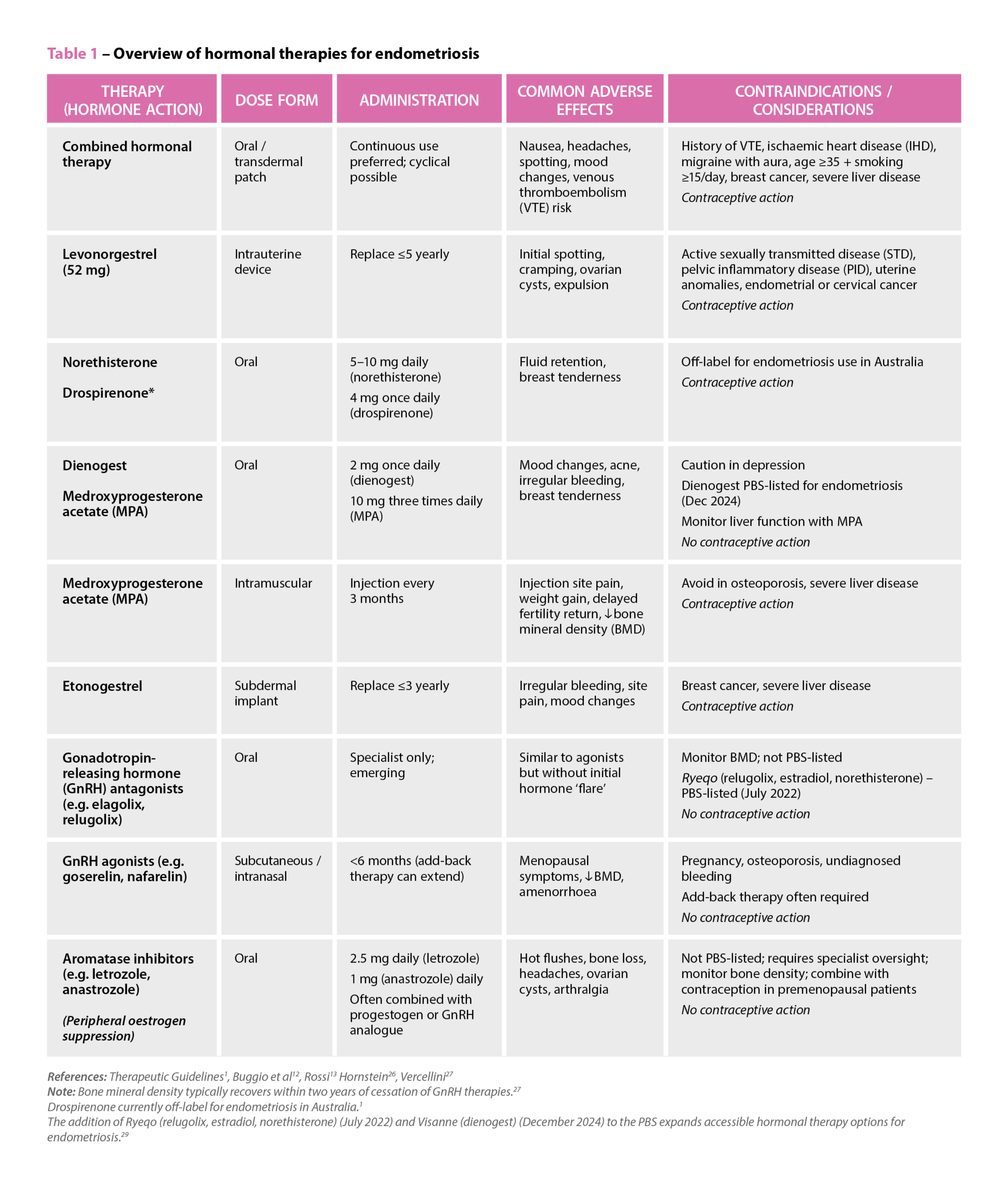 References: Therapeutic Guidelines
References: Therapeutic Guidelines

 Genevieve Adamo MPS (Image: Steve Christo Photography)[/caption]
Genevieve Adamo MPS (Image: Steve Christo Photography)[/caption]

When standard needles for vaccination shortchange patient immunity.
Vaccines are most effective when administered using correct technique – this includes injection site positioning, angle of the needle and needle length.
Most vaccines currently available are administered as intramuscular (IM) injections. With the breadth and depth of pharmacist-administered vaccination growing, it’s timely that pharmacists double check their depth.
What needle size should I use for IM injections?
A 25 mm needle is recommended for most people, including from infants to older adults.
There are two exceptions:
- pre-term infants up to 2 months of age and other very small infants
- very large or obese people.
For very large or obese people, a longer needle of 38 mm length is recommended.1 With 32% of the Australian population being obese,2 around a third of vaccines likely should be administered using longer needles.
What is the risk?
If a needle isn’t long enough, or used at an incorrect angle, the needle may not fully penetrate the deltoid fat pad and therefore be inadvertently administered subcutaneously.
For most vaccines, this risks a higher rate of local adverse events, such as redness, swelling, itching and pain.1,3 This is particularly noted with aluminium-adjuvanted vaccines (such as hepatitis B, dTpa or dT vaccines).2
Concerningly, it is also recognised as reducing immunogenicity.2 For example, Rabipur Inactivated Rabies Virus Vaccine (PCECV) is considered invalid if given subcutaneously.2
Is incorrect needle use widespread?
It’s hard to tell. There is limited contemporary data – and no Australian data was identified when researching this article.
However, overseas studies suggest 38 mm needles are drastically underutilised4 – with one US study suggesting the wrong length needle was used 75% of the time when administering vaccines to obese people.5
What should I do if I accidentally administer a vaccine subcutaneously, instead of into the deltoid muscle?
Consult the Australian Immunisation Handbook.1 The ‘Vaccine injection techniques’ section contains advice on inadvertent subcutaneous injection of intramuscular vaccines.
Error reporting to indemnity insurers and state/territory health department systems may also be required.
In the example of the Rabipur rabies vaccine, as a subcutaneous dose is invalid, the dose must be repeated – an undesirable situation given the cost and time-critical regimen for rabies vaccines.
References
- Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook, Australian Government Department of Health and Aged Care, Canberra, 2022. At: https://immunisationhandbook.health.gov.au/
- Australian Government Australian Institute of Health and Welfare. Overweight and obesity. 2024. At:
www.aihw.gov.au/reports/overweight-obesity/overweight-and-obesity/contents/summary - Mark A, Carlsson RM, Granstrom M. Subcutaneous versus intramuscular injection for booster DT vaccination of adolescents. Vaccine 1999;17(15–16):2067–72. At: https://pubmed.ncbi.nlm.nih.gov/10217608/
- Chhabria S, Stanford FC. A long shot: the importance of needle length in vaccinating patients with obesity against COVID-19. Vaccine 2021;40(1):9–10. At: https://pmc.ncbi.nlm.nih.gov/articles/PMC8580854/
- Palma S, Strohfus P. Are IM injections IM in obese and overweight females? A study in injection technique. Appl Nurs Res 2013;26(4):e1–4. At: https://pubmed.ncbi.nlm.nih.gov/24156877/




