

 Rhiannon Price, Pharmacist at King Edward Memorial Hospital.[/caption]
Rhiannon Price, Pharmacist at King Edward Memorial Hospital.[/caption]
 Caspar Townsend MPS, Pharmacist at Perth Children's Hospital compounding unit[/caption]
Caspar Townsend MPS, Pharmacist at Perth Children's Hospital compounding unit[/caption]
 Iraq Doali, NSW-based locum pharmacist and content creator[/caption]
Iraq Doali, NSW-based locum pharmacist and content creator[/caption]




 Normalisation is medical misogyny and delays diagnosis
Normalisation is medical misogyny and delays diagnosis
 Sharnelle Vella, ABC Radio Melbourne breakfast co-host[/caption]
Sharnelle Vella, ABC Radio Melbourne breakfast co-host[/caption]


 Mike Stephens, Director, Medicines policy and Programs at the National Aboriginal Community Controlled Health Organisation (NACCHO)[/caption]
Mike Stephens, Director, Medicines policy and Programs at the National Aboriginal Community Controlled Health Organisation (NACCHO)[/caption]
 Chastina Heck MPS, Chair of the PSA/NACCHO Aboriginal and Torres Strait Islander Pharmacy Practice Community of Specialty Interest (CSI).[/caption]
Chastina Heck MPS, Chair of the PSA/NACCHO Aboriginal and Torres Strait Islander Pharmacy Practice Community of Specialty Interest (CSI).[/caption]
 Philippa Chigeza, pharmacist at Logan Hospital.[/caption]
Philippa Chigeza, pharmacist at Logan Hospital.[/caption]

Case scenario
Kurt, a 52-year-old slightly overweight electrician, comes into your pharmacy complaining of a burning feeling in his chest after meals, which has persisted for a few weeks.
You ask about other symptoms and he describes a burning sensation behind his sternum, generally mild but worse when he lies down after dinner, and the occasional sour taste in the back of the throat 1–2 times a week. He shares that he eats irregularly, is a heavy coffee drinker due to shift work and often has large late-evening meals. He finds late-night snacking, alcohol and spicy takeaways aggravate his symptoms. Kurt takes no other medicines, has no allergies and is a non-smoker.
Learning objectivesAfter reading this article, pharmacists should be able to:
Competency standards (2016) addressed: 1.1, 1.3, 1.4, 1.5, 2.2, 2.3, 3.1, 3.2, 3.3, 3.5 Accreditation number: PSAAP2605TG Accreditation expiry: 31/03/2028 |
Already read the CPD in the journal? Scroll to the bottom to SUBMIT ANSWERS.
Introduction
As accessible primary healthcare providers, community pharmacists are often the first healthcare provider consulted when a patient presents with symptoms of heartburn, regurgitation or reflux.
Globally, the prevalence of heartburn (retrosternal burning or pain), dyspepsia (indigestion, upper abdomen discomfort) and regurgitation (perception of flow of refluxed stomach content into the mouth or hypopharynx) in adults varies widely. Depending on the definition used and geographical location, prevalence ranges from 2.5% to 52.1%.1
While often asymptomatic, it may result in symptoms caused by refluxate flowing backwards into the oesophagus. This condition, termed gastro-oesophageal reflux (GOR, or simply reflux), is a common physiological event that can occur at any age and is generally considered non-erosive.2
Reflux aetiology involves dysfunction of the lower oesophageal sphincter (LOS) and, in some patients, distal oesophageal motility issues.2,3 A pronounced gastric acid pocket – a highly acidic, unbuffered layer of stomach acid forming on top of food in the upper stomach after a meal, acting as a reservoir that can easily backflow into the oesophagus – significantly contributes to reflux symptoms.4
Other components of gastric juice, such as bile, digestive enzymes and microbial pathogens, can also cause oesophageal symptoms.5-7 Pepsin is an endopeptidase activated at low pH to break down proteins, and can play a pivotal role in damaging the oesophageal surface.5-7 Bile is a digestive fluid designed to break down fats. When bile contacts sensitive mucosa, it can cause painful inflammation and the burning sensation associated with heartburn.5-7 The combination of acid, pepsin and bile can collectively act to assault the oesophageal mucosa.5-7
Gastro-oesophageal reflux disease (GORD) is usually associated with defective LOS function.3 It can cause reflux sufficiently severe to damage mucosa and result in oesophagitis or stricture. A meta-analysis of GORD epidemiology suggested global pooled prevalence of 13.9%.8
Laryngopharyngeal reflux (LPR) occurs when refluxate travels to the throat or higher, and may be the underlying cause of atypical reflux symptoms such as hoarse throat, changes in voice quality, excessive throat clearing and coughing.9 Suspicion of atypical reflux or ‘alarm’ symptoms requires medical referral e.g. cardiac-like chest pain, difficulty swallowing, unintended weight loss, severe abdominal pain, sudden onset reflux symptoms in a person ≥65 years, haematemesis or melaena.3
Symptom presentation
Symptoms across these conditions overlap and do not distinguish non-erosive from erosive pathology, making it difficult to assign a diagnosis without medical investigation such as endoscopy.
As there is no simple, widely accepted screening tool to differentiate between reflux and GORD, and no correlation between the symptom severity and visible changes in the oesophageal mucosa,10 pharmacists must rely on structured history-taking to identify the most appropriate management.
The use of a mnemonic e.g. Chief Complaint History Taking (LOQQSAM),11 together with targeted age or life-event-related questions, are useful to guide symptom description and triage:
- Location (site/radiation)
- Onset
- Quality (character): in the patient’s own words
- Quantity (timing/severity): plus degree of interference with usual daily activities
- Setting
- Associated symptoms
- Modifying factors (aggravating/relieving).
Reflux and GORD management
The aim of empiric reflux therapy is to control symptoms and improve quality of life. This review focuses on non-pregnant adults and young people, with the management approach dependent on symptom frequency and severity. Options include risk reduction and prevention through lifestyle modification and/or pharmacological treatment.
Lifestyle modifications
The pharmacist’s role includes assessing for reflux risk factors, particularly those that are modifiable, and advising on strategies to prevent or reduce risk. Non-pharmacological strategies to reduce reflux symptom frequency or severity in this cohort include12,13:
- maintain a healthy weight through exercise and a balanced diet
- increase physical activity to help gastric motility
- wear comfortable clothing
- avoid reflux-triggering food and drink
- add fibre to the diet e.g. vegetables, legumes, nuts, whole grains
- eat smaller portions, taking time to chew
- learn strategies to manage stress
- reduce or cease smoking and reduce alcohol consumption
- avoid meals and snacks 2–3 hours before bedtime
- elevate the bedhead by 15–20 cm or sleep on the left side if experiencing nocturnal symptoms.
A systematic literature review of clinical trial evidence and clinical practice guidelines14 identified that the strongest levels of evidence for non-pharmacological strategies to improve reflux symptoms were for:
- weight reduction for individuals with a high body mass index (Grade A)
- avoidance or reduction in tobacco smoking (Grade B)
- elevating the bedhead 15–20 cm for nocturnal symptoms (Grade B).
Evidence was categorised with a Grade, based on the National Health and Medical Research Council Levels of Evidence for each study type.15,16
Pharmacological treatment
Most national and international guidelines recommend that a formal diagnostic workup beyond patient history is not required to diagnose the majority of patients who present with upper gastrointestinal symptoms.12,14,17-22
Patient safety is not compromised by typical symptoms of acute reflux (or GORD) being initially managed by pharmacists empirically with a short over-the-counter (OTC) trial of acid suppressant and/or alginate medicines. In Australia, the four OTC therapeutic class options available are: antacids, alginates, histamine-2 receptor antagonists (H2RAs) and proton pump inhibitors (PPIs).
These medicines include:
Antacids
Antacid formulations contain salts of magnesium, aluminium, calcium or sodium. Antacids neutralise hydrochloric acid secreted by gastric parietal cells, leading to increased pH of gastric contents – with potency generally expressed in terms of acid neutralising capacity (ANC).23
However, onset and duration of action depend on the dose forms; powder and liquid have a higher ANC than tablets, and extent of chewing (for tablets). Onset of action is rapid, often less than a minute, with duration of action ranging from 20–60 minutes to up to 2–3 hours, based on whether taken fasting or 1 hour after a meal, respectively.18 So, antacids need to be taken frequently during the day to provide efficient relief of persistent symptoms.
Antacids provide rapid but temporary symptom relief. In 2013, the World Gastroenterology Organisation developed guidelines for the community-based management of common gastrointestinal symptoms – recommending antacids as an appropriate OTC option for infrequent, mild or moderate symptoms of heartburn.12
While updated with a global focus in 2017, antacid +/- alginate therapy remained an empirical recommendation for self-care in ‘countries with limited resources and low Helicobacter pylori prevalence’.13 They generally have a good safety profile when used below the maximum daily dose.19
Most impact on bowel function is dose-related, with calcium and magnesium salts causing diarrhoea and aluminium salts causing constipation.18 However, due to the potential for systemic adverse effects with sodium bicarbonate, regular use should be avoided in older people, those with renal or liver impairment, or those on a sodium-restricted diet.24,25
Alginates/antacid-alginate combinations
Alginates are seaweed-derived, natural polysaccharides.26 Most formulations consist of three chemical components: sodium alginate, sodium bicarbonate and calcium carbonate. The latter two constituents react with stomach acid to yield carbon dioxide and free calcium ions, respectively.27
The combination produces a low-density viscous gel (‘raft’) that floats on top of the stomach contents, forming a physical barrier to reduce or prevent postprandial acid pocket inducing reflux symptoms.27 Alginates can bind bile salts in refluxate, which contributes to their mucoprotective effect.28
Onset of action, symptom relief and duration of action are brand or formulation specific; alginates typically act quickly after administration, and may provide symptom relief for several hours.27–29 Onset of action has been demonstrated to be slower than antacids but faster than either a PPI or H2RA.29 This attribute is particularly useful for nocturnal symptoms and post-meal reflux.
Antacid-alginate combinations have shown to provide rapid and effective relief of mild to moderate reflux symptoms.24
In 2017, Leiman and colleagues30 published a meta-analysis of randomised-controlled trials (RCTs) for treatment of symptomatic GORD (2,095 adult patients – nine studies [N=900] comparing alginate-based products to placebo or antacid, and five studies [N=1195] to PPIs or H2RAs).
Alginate-based products increased the odds of GORD symptom resolution when compared to placebo or antacids (OR:4.42; 95% CI 2.45–7.97), with a moderate degree of heterogeneity between studies (I2=71%, P=0.001). Alginates appeared less effective than PPIs or H2RAs, but the pooled estimate was not statistically significant (OR:0.58; 95% CI 0.27–1.22).30 While, in clinical trials, alginate caused adverse effects with a comparable rate to placebo,30 they are often combined with antacids or contain excipients that may cause adverse effects.
Histamine-2 receptor antagonists (H2RAs)
By blocking the histamine receptor and histamine stimulation of parietal cell acid secretion, H2RAs competitively suppress both stimulated and basal gastric acid secretion induced by histamine.32 H2RAs have good bioavailability.33
Onset of gastric relief is about 60 minutes (decreasing stomach acid production within 1 to 3 hours), with a dose-dependent duration of action of 4 to 12 hours.34 Although less effective than PPIs, H2RAs are useful for mild and/or intermittent symptoms or when PPIs are unsuitable.17,19 Ranitidine is the only H2RA available in short-course Schedule 2 packs, while others are Schedule 4, restricting OTC H2RA options.
Proton pump inhibitors (PPIs)
PPIs are the most potent OTC acid suppression therapy available.21 They are acid-labile pro-drugs. As food can decrease bioavailability, PPIs are best taken on an empty stomach, once daily 30–60 minutes before breakfast.19 Proton pumps become activated during meals, and administration prior to food intake will enhance efficacy.18,19
PPIs are selectively taken up by gastric parietal cells and concentrated within the acidic canalicular space where they become protonated and convert to an active sulfenamide form. The activated compound then covalently binds to cysteine residues on the luminal surface of the hydrogen/potassium ATPase.
By irreversibly inactivating this proton pump, PPIs suppress both basal and stimulated gastric acid secretion. Acid production remains reduced until new pumps are synthesised, a process that may take up to 36 hours.35
Once absorbed, onset of action is about 90 minutes.36 While PPIs have a short elimination half-life (1–2 hours), their pharmacodynamic effect to reliably maintain intragastric pH >4 can last 15 to 21 hours, due to their irreversible covalent bonding to the proton pump. This provides symptom relief for 24 hours or longer, after 1 to 3 days of treatment.37,38
The delay between PPI initiation and inhibition of acid secretion reaching steady state means that patients with frequent reflux symptoms may benefit from concomitant therapy with an agent that provides short-term relief, such as an antacid-alginate, while waiting for the PPI to take effect. Additionally, by co-localising to the postprandial acid pocket to create a mechanical barrier that suppresses gastric reflux at the LOS, and binding bile salts to contribute to the mucoprotective effect, antacid-alginates may be considered as adjunctive therapy in some patients with breakthrough symptoms, and in PPI deprescribing to help manage symptom rebound.39,40
OTC PPIs are indicated for the initial relief of reflux and GORD as:
- once daily for 7 days (except for esomeprazole that can be supplied up to 14 days as a Pharmacy Only medicine)
- once daily for up to 14 days as a Pharmacist Only medicine, excluding esomeprazole as there is no option available.
In contrast, aligned with the Therapeutic Guidelines (TG), pharmacists approved for expanded scope can prescribe 4 weeks of ‘standard dose’ PPI (esomeprazole 20 mg, lansoprazole 30 mg, omeprazole 20 mg pantoprazole 40 mg or rabeprazole 20 mg), 0.5–1 hour before a meal.17
In RCTs, 2–4-weeks of PPIs at doses approved for OTC use are usually effective in the management of those with frequent reflux symptoms.37,42,43 A non-response to a short course of acid-suppressive therapy warrants prompt medical consultation, as it can suggest other diagnoses.
Globally, guideline differences in pharmacist empirical adult management of reflux or GORD largely stem from regulatory limitations, differences in definition of symptom severity and frequency, and whether used for initial or maintenance therapy.
TG recommendations include OTC and prescription options from all four reflux medicines classes. For mild, intermittent symptoms (specified as 1–2 episodes weekly), options are an antacid-alginate, combined magnesium-aluminium antacid or H2RA (all when necessary), or standard dose PPI once daily.17
For frequent or severe typical GORD symptoms, TG recommend a 4–8 week initial course of standard dose PPI; then when symptom control is adequate, step down to maintenance therapy (second daily or half the daily dose to therapy only on days when symptoms arise).17
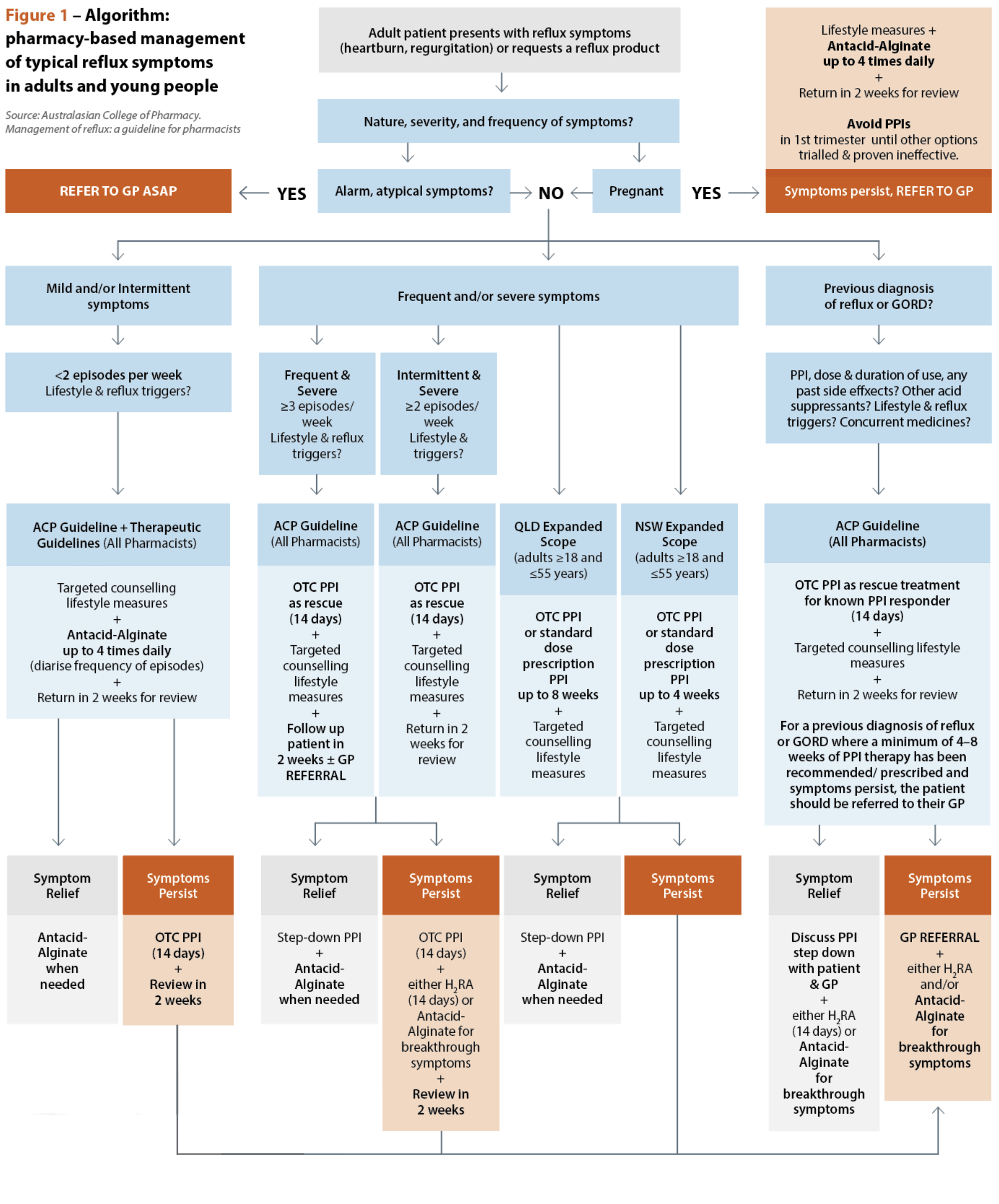
Unfortunately, TG does not provide guidance when reflux (not GORD) symptoms are more frequent or severe. The Australasian College of Pharmacy guidelines attempt a more nuanced, pharmacist-focused approach to initial management (Figure 1).14
 Irrespective of approach, there is general consensus that13,14, 17-19:
Irrespective of approach, there is general consensus that13,14, 17-19:
Adults and young people with reflux symptoms trial diet and lifestyle modifications; in those with mild symptoms, this may be sufficient.
Multimodal pharmacological management options address the variability of reflux symptom frequency and severity, with a potential role for antacid-alginates during PPI initiation, and for intermittent breakthrough symptoms while taking or stepping down from a PPI.
Pharmacists should discuss treatment options, potential benefits, harms, and logistics for correct use, together with the patient’s preferences, so the decision to proceed is collaborative.
Pharmacists should also advise the patient to return after 2–4 weeks for review and potential step-down therapy, with symptoms or signs requiring return to the pharmacist or general practitioner discussed.
Where patients experience a poor response to a standard dose OTC PPI, or typical reflux symptoms co-exist with ‘alarm’ or atypical symptoms of concern – medical referral to exclude the presence of a serious condition is imperative.
Expanded scope
Australian pharmacists are expanding their scope of practice, with full scope of practice gaining momentum. In 3 years, the vision has evolved from a 2022 Queensland Government election commitment to work with pharmacy stakeholders to design and implement a pilot of pharmacists practicing to their full scope (the Queensland Community Pharmacy Scope of Practice Pilot) to business-as-usual community pharmacy prescribing services.
Since 1 July 2025, pharmacists completing additional training and meeting the requirements of the Extended Practice Authority have been able to provide clinical advice and treatment, which may include prescribing medicines to adults (18–55 years) for a range of specified acute common conditions, in accordance with a tailored clinical practice guideline.44
NSW Health has also introduced Practice Standards (adults ≥18 to ≤50 years) for expanded pharmacist scope, informed by the Queensland Health clinical practice guidelines and NSW Health emergency care assessment and treatment protocols. It is hoped that a national approach will follow, as other states roll out extended scope services.45 Both jurisdictions list gastro-oesophageal reflux and GORD as an included condition and service, with a companion clinical practice guideline and Practice Standard, respectively.46,47
All pharmacists should take advantage of these reflux resources as they provide an evidence-informed framework for patient assessment and management, primarily aligned to the TG.16 Additional expanded scope training is beneficial to improve pharmacists’ clinical skills and confidence. However, a quality and consistent approach to clinical assessment, triage, and referral is embedded in the competency standards for all pharmacists.48
While extended scope imposes formal responsibilities for patient consultation, documentation and follow-up – pharmacists should undertake these quality care strategies. The main prescribing advantages of expanded scope is extending the initial standard dose PPI treatment period from 2–4 weeks, and, in Queensland, access to Schedule 4 H2RAs. Importantly, the Clinical Practice Guideline and Practice Standard both focus heavily on the use of non-pharmacological and management options in reflux symptom management.
Knowledge to practice
Pharmacists play a key role in assessing reflux symptoms through structured history-taking, identifying red flags, and selecting appropriate non-pharmacological and pharmacological options based on symptom frequency and severity. Judicious use of antacid–alginate therapy for rapid relief and adjunctive support during PPI initiation or step-down can optimise symptom control while promoting safe, evidence-based self-management.
Conclusion
Effective management of reflux and GORD in pharmacy practice requires a patient-centred approach that integrates lifestyle modification with tailored use of OTC and, where appropriate, expanded-scope prescribing options. By applying current guidelines and supporting timely review and referral, pharmacists can improve symptom outcomes and quality of life.
Case scenario continuedYou explain to Kurt that his lifestyle is likely contributing to his symptoms and offer targeted counselling to reduce modifiable risks. You provide an OTC PPI once daily, taken 30–60 minutes before his first daily meal for 14 days, and an antacid-alginate, to use for 1–3 days before the PPI starts to work and for breakthrough symptoms, especially at night, when needed. You make an appointment with him to return in 2 weeks to check his progress, or earlier to you or his GP if symptoms worsen. At review, Kurt says he is much improved by his medicines and is avoiding his reflux triggers, especially raising the bedhead. He is happy to step-down to use of antacid-alginate when needed, and return if his symptoms worsen in the future. |
This article is accredited for group 2 CPD credits. Click submit answers to complete the quiz and automatically record CPD against your record.
If you do get an enrolment error, please click here![]()
Key points
- Structured history-taking is required to guide empirical management and identify indications for referral.
- Management combines lifestyle modification with stepwise, evidence-based use of antacids, alginates and acid-suppressive therapy, with review and step-down.
- Antacid–alginate therapy has a defined role for rapid symptom relief and as adjunctive treatment during initiation or step-down of PPI therapy.
References
- Eusebi LH, Ratnakumaran R, Yuan Y et al. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut. 2018;67(3):430-40. doi: 10.1136/gutjnl-2016-313589
- DeVault KR. Review article: the role of acid suppression in patients with non-erosive reflux disease or functional heartburn. Aliment Pharmacol Ther 2006;23 Suppl 1:33-9. doi: 10.1111/j.1365-2036.2006.02798.x.
- Vakil N, van Zanten SV, Kahrilas P, et al; Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol 2006;101(8):1900-20. doi: 10.1111/j.1572-0241.2006.00630.x.
- Kahrilas PJ, McColl K, Fox M, et al. The acid pocket: a target for treatment in reflux disease? Am J Gastroenterol. 2013;108(7):1058-1064.
- Bardhan KD, Strugala V, Dettmar PW. Reflux revisited: advancing the role of pepsin. Int J Otolaryngol 2012:646901. doi: 10.1155/2012/646901.
- Lee YY, Woodman HL. Pepsin: An oesophageal irritant in the perception of reflux disease. In DA Johnson, ed. In Gastroesophageal reflux disease: From pathophysiology to treatment. (pp. 55-72). InTech Open 2013: 55-72. doi: 10.5772/55589.
- Tack J. Review article: the role of bile and pepsin in the pathophysiology and treatment of gastro-oesophageal reflux disease. Aliment Pharmacol Ther 2006;24 Suppl 2:10-6. doi: 10.1111/j.1365-2036.2006.03040.x.
- Nirwan JS, Hasan SS, Babar ZU, et al. Global prevalence and risk factors of gastro-oesophageal reflux disease (GORD): Systematic review with meta-analysis. Sci Rep 2020;10(1):5814. doi: 10.1038/s41598-020-62795-1.
- Campagnolo AM, Priston J, Thoen RH, et al. Laryngopharyngeal reflux: diagnosis, treatment, and latest research. Int Arch Otorhinolaryngol 2014 Apr;18(2):184-91. doi: 10.1055/s-0033-1352504
- Stanghellini V, Cogliandro R, Cogliandro L, et al. Unsolved problems in the management of patients with gastroesophageal reflux disease. Dig Liv Dis 2003;35(12):843–8. doi: 10.1016/j.dld.2003.09.003
- Chapter 2: Obtaining a patient history. In: Herrier R, Apgar D, Boyce R, Foster SL (eds). Patient assessment in Pharmacy. McGraw-Hill Education, 2015.
- Hunt R, Quigley E, Abbas Z, et al; World Gastroenterology Organisation. Coping with common gastrointestinal symptoms in the community: a global perspective on heartburn, constipation, bloating, and abdominal pain/discomfort. J Clin Gastroenterol. 2014;48(7):567-78. doi:
- Hunt R, Armstrong D, Katelaris P, et al; Review Team. World Gastroenterology Organisation global guidelines: GERD global perspective on gastroesophageal reflux disease. J Clin Gastroenterol 2017;51(6):467-78. doi: 10.1097/MCG.0000000000000854.
- McGuire TM, Nash S. Management of reflux: a guideline for pharmacists. Australasian College of Pharmacy. July 2024:1-117. [Cited 2025 Dec 29] Available at: https://www.acp.edu.au/education/guidelines/gastroesophageal-reflux/
- National Health and Medical Research Council. NHMRC levels of evidence and grades for recommendations for guideline developers. Canberra: NHMRC, 2009. Available at: / Additional levels of evidence and grades for recommendations for developers of guidelines 2008-2010
- Andrews JC, Schünemann HJ, Oxman AD, et al. GRADE guidelines: 15. Going from evidence to recommendation-determinants of a recommendation’s direction and strength. J Clin Epidemiol 2013; 66(7):726-35. doi: 10.1016/j.jclinepi.2013.02.003.
- Gastro-oesophageal reflux in adults. Therapeutic Guidelines; [updated Feb 2025]. At: Home | Therapeutic Guidelines
- Sanson LN, ed. Gastro-oesophageal reflux. Australian pharmaceutical formulary and handbook (APF). 26th edn. Canberra: Pharmaceutical Society of Australia; 2024.
- Rossi S. Buckley N ed. Gastro-oesophageal reflux disease. In: AMH. Adelaide. Australian Medicines Handbook Pty Ltd; [updated Jan 2026]. At: Gastro-oesophageal reflux disease – Australian Medicines Handbook
- Koop H, Fuchs KH, Labenz J, et al. S2k guideline: gastroesophageal reflux disease guided by the German Society of Gastroenterology: AWMF register no. 021-013. Z Gastroenterol. 2014;52(11):1299-346. German. doi: 10.1055/s-0034-1385202
- Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 2013;108(3):308-28. quiz 329. doi: 10.1038/ajg.2012.444.
- Baldi F, Crotta S, Penagini R. Guidelines for the diagnostic and therapeutic management of patients with gastro-oesophageal reflux disease. A position statement of The Italian Association of Hospital Gastroenterologists (AIGO), Italian Society of Gastrointestinal Endoscopy (SIED), and Italian Society of Gastroenterology (SIGE). Ital J Gastroenterol Hepatol 1998;30(1):107-12.
- Dolberg MK, Nielsen LP, Dahl R. Pharmacokinetic profile of oral magnesium hydroxide. Basic Clin Pharmacol Toxicol 2017;120(3):264-9. doi: 10.1111/bcpt.12642.
- Goh KL, Lee YY, Leelakusolvong S, et al. Consensus statements and recommendations on the management of mild-to-moderate gastroesophageal reflux disease in the Southeast Asian region. JGH Open 2021;5(8):855-63. doi: 10.1002/jgh3.12602
- Garg V, Narang P, Taneja R. Antacids revisited: review on contemporary facts and relevance for self-management. J Int Med Res. 2022 Mar;50(3):3000605221086457. doi: 10.1177/03000605221086457.
- Abka-Khajouei R, Tounsi L, Shahabi N, et al. Structures, properties and applications of alginates. Mar Drugs 2022;20(6):364. doi: 10.3390/md20060364.
- Dettmar PW, Gil-Gonzalez D, Fisher J, et al. A comparative study on the raft chemical properties of various alginate antacid raft-forming products. Drug Dev Ind Pharm 2018;44(1):30-9. doi: 10.1080/03639045.2017.1371737.
- Strugala V, Avis J, Jolliffe IG, et al The role of an alginate suspension on pepsin and bile acids – key aggressors in the gastric refluxate. Does this have implications for the treatment of gastro-oesophageal reflux disease? J Pharm Pharmacol 2009;61(8):1021-8. doi: 10.1211/jpp/61.08.0005.
- Dettmar PW, Sykes J, Little SL, et al. Rapid onset of effect of sodium alginate on gastro-oesophageal reflux compared with ranitidine and omeprazole, and relationship between symptoms and reflux episodes. Int J Clin Pract 2006; 60(3): 275–83. doi: 10.1111/j.1368-5031.2006.00800.x.
- Leiman DA, Riff BP, Morgan S, et al. Alginate therapy is effective treatment for GERD symptoms: a systematic review and meta-analysis. Dis Esophagus 2017 1;30(5):1-9. doi: 10.1093/dote/dow020.
- Zhao CX, Wang JW, Gong M. Efficacy and safety of alginate formulations in patients with gastroesophageal reflux disease: a systematic review and meta-analysis of randomized controlled trials. Eur Rev Med Pharmacol Sci 2020;24(22):11845-857. doi: 10.26355/eurrev_202011_23841
- MacFarlane B. Management of gastroesophageal reflux disease in adults: a pharmacist’s perspective. Integr Pharm Res Pract. 2018;7:41-52.
- Yeomans ND. Drugs that inhibit acid secretion. Aust Prescr 2000;23:57-9. doi: 10.18773/austprescr.2000.071
- Netzer P, Brabetz-Höfliger A, Bründler R et al. Comparison of the effect of the antacid Rennie versus low-dose H2-receptor antagonists (ranitidine, famotidine) on intragastric acidity. Aliment Pharmacol Ther 1998;12(4):337-42. doi: 10.1046/j.1365-2036.1998.00316.x
- Shin JM, Sachs G. Pharmacology of proton pump inhibitors. Curr Gastroenterol Rep 2008;10(6):528-34. doi: 10.1007/s11894-008-0098-4
- Bate CM, Green JR, Axon AT, et al. Omeprazole is more effective than cimetidine for the relief of all grades of gastro-oesophageal reflux disease-associated heartburn, irrespective of the presence or absence of endoscopic oesophagitis. Aliment Pharmacol Ther 1997;11(4):755-63. doi: 10.1046/j.1365-2036.1997.00198.x.
- Allgood, Grender JM, Shaw MJ, et al. Comparison of Prilosec OTC (omeprazole magnesium 20.6 mg) to placebo for 14 days in the treatment of frequent heartburn. J Clin Pharm Ther 2005;30(2):105–12. doi: 10.1111/j.1365-2710.2004.00620.x.
- Miner P Jr, Katz PO, Chen Y, et al. Gastric acid control with esomeprazole, lansoprazole, omeprazole, pantoprazole, and rabeprazole: a five-way crossover study. Am J Gastroenterol 2003;98(12): 2616–20. doi: 10.1111/j.1572-0241.2003.08783.x.
- Reimer C, Lødrup AB, Smith G, et al. Randomised clinical trial: alginate (Gaviscon Advance) vs. placebo as add-on therapy in reflux patients with inadequate response to a once daily proton pump inhibitor. Aliment Pharmacol Ther 2016;43(8):899-909. doi: 10.1111/apt.13567.
- Coyle C, Crawford G, Wilkinson J, et al. Randomised clinical trial: addition of alginate-antacid (Gaviscon Double Action) to proton pump inhibitor therapy in patients with breakthrough symptoms. Aliment Pharmacol Ther 2017;45(12):1524-33. doi: 10.1111/apt.14064
- Vales A, Coyle C, Plehhova K. Randomised clinical trial: the use of alginates during preinvestigation proton pump inhibitor wash-out and their impact on compliance and symptom burden. BMJ Open Gastroenterol 2023;10(1):e001026. doi: 10.1136/bmjgast-2022-001026. K
- Kushner PR, Snoddy AM, Gilderman L, et al. Lansoprazole 15 mg once daily for 14 days is effective for treatment of frequent heartburn: results of 2 randomized, placebo-controlled, double-blind studies. Postgrad Med 2009;121(4):67-75. doi: 10.3810/pgm.2009.07.2019.
- Peura DA, Traxler B, Kocun C, et al. Esomeprazole treatment of frequent heartburn: two randomized, double-blind, placebo-controlled trials. Postgrad Med 2014;126(4):33-41. doi: 10.3810/pgm.2014.07.2781.
- Queensland Health. Community pharmacy prescribing in Queensland. 2025. At: https://www.health.qld.gov.au/clinical-practice/guidelines-procedures/community-pharmacy-pilots
- Pharmaceutical Services, NSW Health. Additional services from Queensland-trained pharmacists – information for pharmacists. 2025. At: https://www.health.nsw.gov.au/pharmaceutical/Pages/additional-services-pharmacists.aspx
- Queensland Health. Queensland Community Pharmacy Gastro-oesophageal Reflux and Gastro-oesophageal Reflux Disease – Clinical Practice Guideline. 2025. At: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.health.qld.gov.au/__data/assets/pdf_file/0019/1304245/gastro-oesophageal-guideline.pdf
- NSW Health. NSW Pharmacist Practice Standards for gastro-oesophageal reflux and gastro-oesophageal reflux disease. 2025 At: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.health.nsw.gov.au/pharmaceutical/Documents/practice-standards-gastro-reflux.pdf
- Pharmaceutical Society of Australia. Professional Practice Standards 2023 Version 6 [Internet]. Canberra, ACT (Deakin West): Pharmaceutical Society of Australia. 2023. At: www.pharmacyboard.gov.au
Our author
Dr Treasure McGuire is Assistant Director of Pharmacy at Mater Health in South-East Queensland, Associate Professor of Pharmacology, Faculty of Health Sciences and Medicines at Bond University and Honorary Associate Professor in the School of Pharmacy and Pharmaceutical Sciences at the University of Queensland.
Our reviewer
Sharon Ambalal MPH BPharm MPS



