



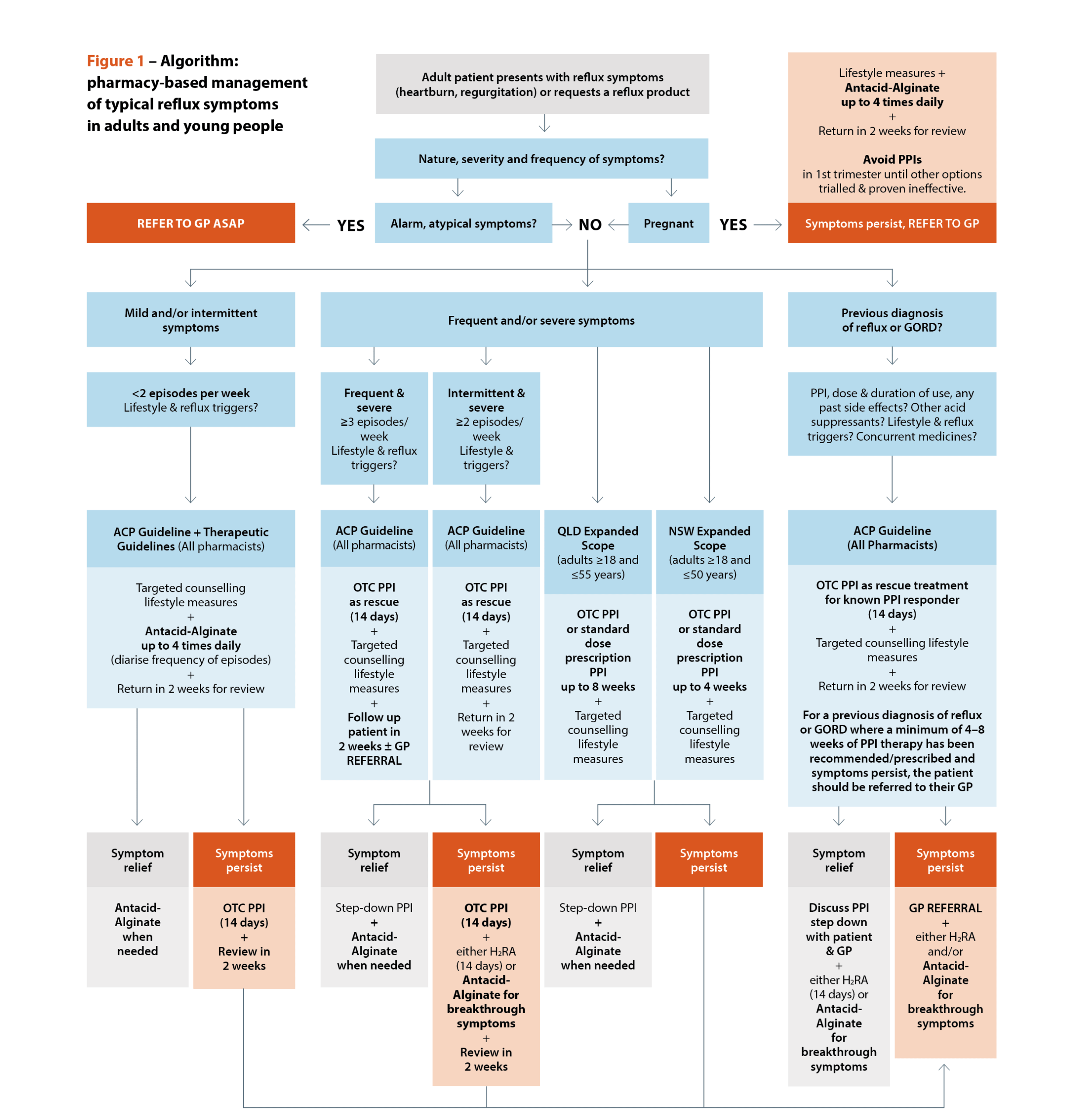
 Sources: Australasian College of Pharmacy. Management of reflux: a guideline for pharmacists. Queensland Health. Queensland Community Pharmacy Gastro-oesophageal Reflux and Gastro-oesophageal Reflux Disease – Clinical Practice Guideline. NSW Health. NSW Pharmacist Practice Standards for gastro-oesophageal reflux and gastro-oesophageal reflux disease.[/caption]
Sources: Australasian College of Pharmacy. Management of reflux: a guideline for pharmacists. Queensland Health. Queensland Community Pharmacy Gastro-oesophageal Reflux and Gastro-oesophageal Reflux Disease – Clinical Practice Guideline. NSW Health. NSW Pharmacist Practice Standards for gastro-oesophageal reflux and gastro-oesophageal reflux disease.[/caption]

 Dr Ming S Soh PhD, BPharm (Hons)[/caption]
Dr Ming S Soh PhD, BPharm (Hons)[/caption]



A good night’s sleep

References
1. Hillman D, Mitchell S, Streatfeild J, et al. The economic cost of inadequate sleep. Sleep 2018;41(8). Epub 2018 Jun 4.
2. Claughton D. Farmers...
Are unconscious gender biases widening the Australian gender pain gap?
References
Filingim R. Individual differences in pain: understanding the mosaic that makes pain personal. Pain 2017;158(Suppl 1):S11–S18.
Widemann TH, Edwards RR, Walton DM, et...
Denosumab for erosive hand osteoarthritis
References
Favero M, Belluzzi E, Ortolan A, et al. Erosive hand osteoarthritis: latest findings and outlook. Nat Rev Rheumatol 2022;18(3):171–83.
Kloppenburg M, Kroon F....
Maria Berbecaru extended interview
Just 3 years out of university, in 2019 Maria Berbecaru MPS made history by implementing Australia's first integrated community pharmacy-delivered medicine supply and on-site...
Why is my PPI not working?
References
Gastro-oesophageal reflux in adults . In: Therapeutic Guidelines. Melbourne: Therapeutic Guidelines Limited. At: www.tg.org.au
Daniels B, Schaffer A, Buckley NA, et al. The...
Credentialed in the country

Natasha Downing is a credentialed pharmacist who loves volunteering, kicking a football with her family, and playing with their dog Rosie.
