

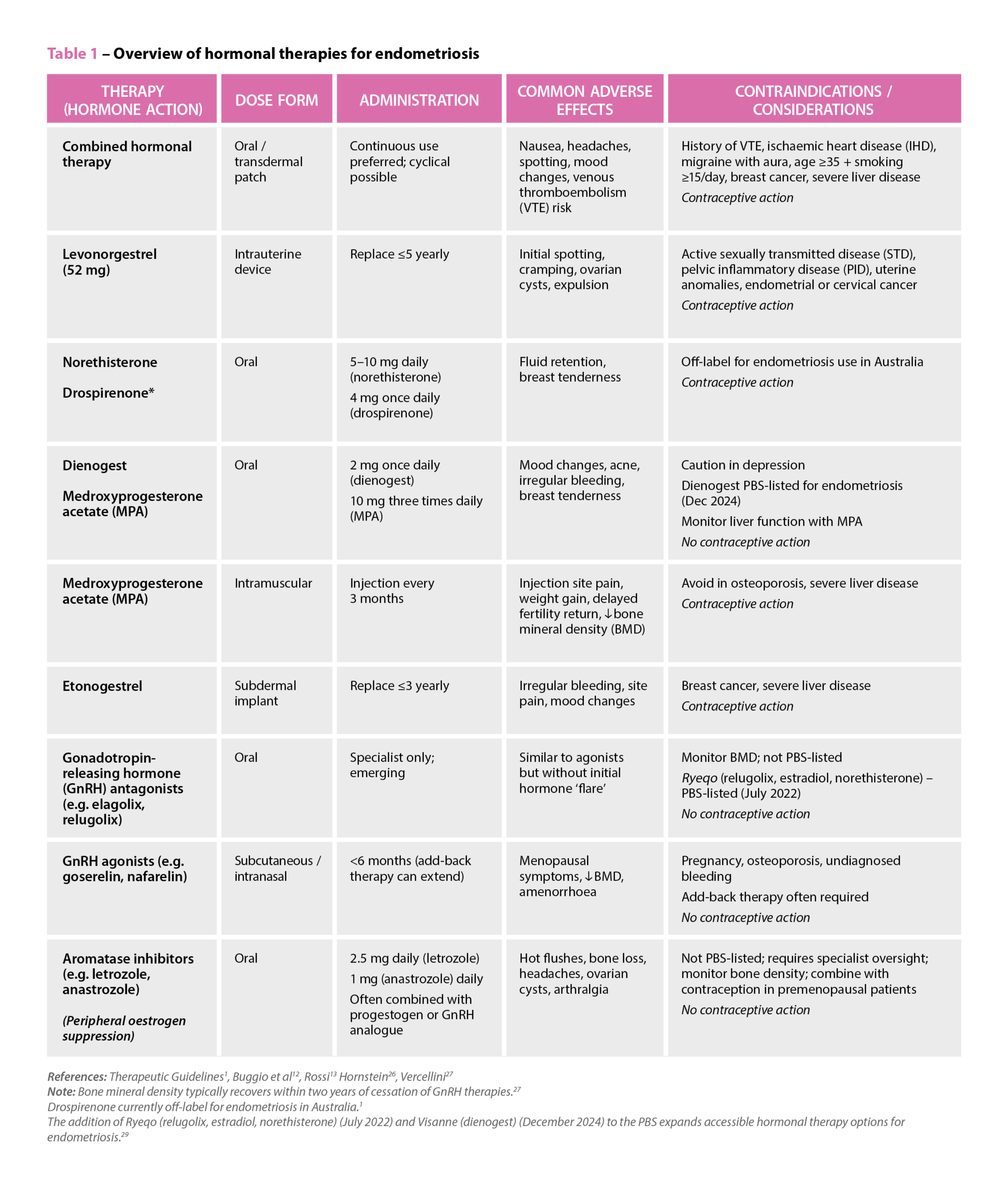
 References: Therapeutic Guidelines
References: Therapeutic Guidelines

 Genevieve Adamo MPS (Image: Steve Christo Photography)[/caption]
Genevieve Adamo MPS (Image: Steve Christo Photography)[/caption]



Tobacco use is the leading cause of preventable morbidity and mortality in Australia and worldwide.
It is responsible for 7 million deaths annually, including an estimated 1.6 million non-smokers who are exposed to second-hand smoke. All forms of tobacco use are harmful, and there is no safe level of exposure. Cigarette smoking is the most common form of tobacco use worldwide, with examples of other types of products including waterpipe tobacco, cigars, cigarillos, heated tobacco, roll-your-own tobacco, pipe tobacco, bidis and kreteks, and smokeless tobacco products.1
The prevalence of daily smoking in Australia has declined from 24% in 1991 to 11% in 2019, attributed to the public health campaigns such as plain packaging and price increases. However, its prevalence remains high in some people; for example, those with harmful or dependent use of other substances (66%), or those with serious mental illness and related conditions (62%).2
Tobacco use, driven by nicotine dependence, is chronic and relapsing. While more than half of all people who smoke try to change their smoking behaviour every year,2 fewer than 1 in 10 adults who smoke will succeed in quitting each year.3 Most individuals will not be able to make long-term changes without treatment.2
The most effective approach for managing smoking and nicotine dependence is the combination of behavioural interventions and pharmacotherapy. Examples of behavioural interventions can include tailored counselling, cognitive behavioural therapy, acceptance and commitment therapy, and motivational interviewing.2 First-line options for pharmacotherapy include nicotine replacement therapy, varenicline and bupropion. Nicotine replacement therapy can be safely added to varenicline or bupropion if required, but data is still lacking on combining bupropion with varenicline.2 If one first-line drug therapy is not suitable or effective after an adequate trial, then the recommendation is to consider another first-line drug before considering nortriptyline or nicotine vaping products (second-line options).2 So while options are available, not everyone responds to them, and relapse rates are high.
There has been interest, in the use of glucagon-like peptide-1 (GLP-1) analogues in treating various forms of addiction, including food, alcohol, opioid and nicotine addiction, and whether it can be used to help people addicted to gambling, sex, shopping and so on,
by influencing the brain’s dopamine pathways related to motivation, pleasure and reward.4
Table: Semaglutie dosing information (AMH)7
| CONDITION | DOSING (ADULT), SUBCUTANEOUSLY |
| Type 2 diabetes – Ozempic | Initially 0.25 mg once a week for 4 weeks, then increase to 0.5 mg once a week. If required, after at least another 4 weeks, increase to 1 mg once a week. |
| Weight management – Wegovy | Initially 0.25 mg once a week for 4 weeks, then 0.5 mg once a week for 4 weeks, then 1 mg once a week for 4 weeks, then 1.7 mg once a week for 4 weeks, then (if tolerated) maintenance dose 2.4 mg once a week. |
| Tobacco use disorder (nicotine dependence)* | As per dose for diabetes. |
* Semaglutide does not have an indication for this condition – dose provided is indicative only
A recently published study looked at the association of semaglutide with tobacco use disorder related healthcare measures in people with type 2 diabetes.5 Epidemiological studies reportedly suggest a prevalence of 20.8% among individuals with type 2 diabetes.6 Cessation of tobacco use in people with type 2 diabetes is important, as cigarette smoking further increases the risk of cardiovascular disease, peripheral vascular disease and neuropathy. Semaglutide is of course widely known for its use in type 2 diabetes, and for weight management, by being an analogue of GLP-1 (an incretin), increasing glucose-dependent insulin secretion, suppressing inappropriate glucagon secretion, and delaying gastric emptying, which slows glucose absorption and decreases appetite.7
The study6 used an emulation target trial design, using observational data to emulate a target trial by applying principles of randomised trials to estimate a causal effect of an intervention. It compared the new use of semaglutide against seven other diabetes medicines (insulins, metformin, dipeptidyl-peptidase-4 inhibitors, sodium-glucose cotransporter-2 inhibitors, sulfonylureas, thiazolidinediones, and other GLP-1RAs), and looked at healthcare measures such as medical encounter for diagnosis of tobacco use disorder, smoking cessation medication prescriptions, and smoking cessation counselling within a 12-month follow-up period.6 Looking across a nationwide database of patient electronic health records in the US from December 2017 to March 2025, the authors found 222,942 new users of diabetes medicines, of which 5,967 were semaglutide.
Semaglutide was associated with a significantly lower risk for medical encounters, particularly compared to insulin, for tobacco use disorder diagnosis compared with other medicines for diabetes (HR, 0.68 [95% CI, 0.63–0.74]), smoking cessation prescriptions (HR, 0.32 [CI, 0.28–0.38]), and counselling (HR, 0.32 [CI, 0.28–0.38]), regardless of whether the person had a diagnosis of obesity.6
While these findings are interesting and promising, the current study data draws from electronic health records, which can be affected by documentation bias, residual confounding or missing data. The authors also point out they did not measure granular details such as current nicotine intake and smoking, or the number of cigarettes per day, changes in cravings, or duration of time to take up smoking again, as a reduction in the encounters measured by the study could be due to a reduction in tobacco use, or a relapse; and successful quitting with assistance was also not captured.
Dedicated, large-scale randomised controlled trials over longer periods of follow-up are needed, the authors have concluded.6
References
- World Health Organisation. Tobacco Geneva, Switzerland: World Health Organisation. 2025. At: www.who.int/news-room/fact-sheets/detail/tobacco
- Addiction Expert Group. Overview of tobacco smoking and nicotine dependence. 2023. Melbourne (AU): Therapeutic Guidelines Ltd. At: www.tg.org.au
- US Centers for Disease Control and Prevention. Smoking Cessation: Fast Facts US: US Centers for Disease Control and Prevention. 2024 At: www.cdc.gov/tobacco/php/data-statistics/smoking-cessation/index.html#:~:text=the%20past%20year.-,Less%20than%201%20in%2010%20adults%20who%20smoke%20cigarettes%20succeed,smoking%20in%20the%20past%20year
- Conley M. Five things to know about GLP-1s and addiction US: Standford Medicine. 2023. At: https://med.stanford.edu/news/insights/2025/04/ozempic-addiction-glp-1s-mounjaro-lembke.html
- Wang W, Volkow N, Berger N, et al. Association of semaglutide with tobacco use disorder in patients with type 2 diabetes: target trial emulation using real-world data. Ann Intern Med 2024;177(8):1016–27.
- Popovic D, Patoulias D, Koufakis T, et al. Semaglutide and smoking cessation in individuals with type 2 diabetes mellitus: there is no smoke without fire! Expert Rev Clin Pharmacol. 2024;17(11):1009–12.
- Australian Medicines Handbook online [Internet]. Doxycycline. 2025. Adelaide (AU): Australian Medicines Handbook Pty Ltd. At: https://amhonline.amh.net.au/auth




