Should I use label 10b if aspirin has been prescribed?
- SHARE
-

-

-

- SHARE
-
-
-


td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29793
[post_author] => 3410
[post_date] => 2025-06-30 12:58:25
[post_date_gmt] => 2025-06-30 02:58:25
[post_content] => This week pharmacists will see a suite of regulatory and funding changes take effect.
Here are the six key updates pharmacists need to know before tomorrow.
1. Dispensing fees will marginally rise
Under the Eighth Community Pharmacy Agreement, pharmacists’ dispensing fee – along with the Tier 1 Administration, Handling and Infrastructure fee and the Dangerous Drug fee – will be indexed by the Consumer Price Index (CPI) annually on 1 July.
Over the past 12 months to the March 2025 quarter, the CPI increased to 2.4%.
So from tomorrow, there will be a slight jump in the per script dispense fee, which will rise from $8.67 to $8.89.
2. (Dis)continued dispensing as emergency measures roll back
As of tomorrow, temporary emergency measures that expanded the range of medicines available under Pharmaceutical Benefits Scheme (PBS) Continued Dispensing arrangements will be repealed.
The emergency authority which authorised these Continued Dispensing arrangements for private and PBS prescriptions in New South Wales, will also end at 11:59 pm tonight.
Only the standard list of 149 PBS-listed molecules will be available under Continued Dispensing in most jurisdictions, covering conditions such as asthma, diabetes, heart disease, high cholesterol and HIV.
However, Continued Dispensing will continue for some. Just enacted in Queensland, the amount of medicine a pharmacist can supply to a patient as an ‘emergency supply’ is increasing from 3 days’ supply to the smallest available manufacturer’s pack of the medicine. This applies in addition to the supply provisions enabled under the Commonwealth Continued Dispensing Determination. And in Tasmania permanent regulation also allows full Continued Dispensing as private supply for all Prescription Only Medicines.
A full list of what’s happening in your state or territory is available via PSA’s Regulation Hub which will be updated overnight to reflect these changes.
The PSA has long advocated for the full measure to be made permanent across the nation.
‘We’ve seen temporary continued dispensing measures introduced during natural disasters, which is important, but there are several scenarios where a permanent policy would help patients, from personal emergencies to natural disasters,’ said PSA CEO Adjunct Associate Professor Steve Morris.
‘PSA is again urging the federal government to work with state and territory governments to permanently protect emergency access to medicines.’
3. New vaping standards will come into effect
From 1 July, the Therapeutic Goods Administration (TGA) will implement strengthened standards for all therapeutic nicotine vaping products used for smoking-cessation and nicotine-dependence. This measure is designed to mitigate risks associated with therapeutic vaping products and ensure a consistent level of safety and quality across all products supplied through pharmacies.
Under the new standards, pharmacies will only be permitted to supply vapes that satisfy defined criteria around permitted ingredients, tamper-evident and child-resistant packaging, and clear, consistent labelling.
Pharmacists should refer to the TGA’s notified vape list, which details all therapeutic vaping products approved for smoking cessation and the management of nicotine dependence.
4. Pharmacists now have longer to transition to the new MMR and ACOP credential
Until recently, pharmacists were required to meet the revised credentialing standards by 30 June 2025 – either by obtaining Recognition of Prior Learning (RPL) towards their new credential or by undertaking further education to fulfil the updated requirements.
The deadlines to achieve both credentials have now been extended to:

td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29777
[post_author] => 235
[post_date] => 2025-06-27 09:36:24
[post_date_gmt] => 2025-06-26 23:36:24
[post_content] => Decision-support tools are designed to promote patient safety. But when here's a pop-up for everything, the message can be diluted.
We all know the feeling. You’re in the middle of something – maybe deep into a busy shift in the pharmacy, or on the wards in the hospital, or even scrolling on your phone at home – and another pop-up appears.
You’ve seen it before, so your instinct is to dismiss it without a second thought.
While ignoring the latest alert from your fitness app might mean falling behind on your step count, dismissing a decision-support pop-up in a healthcare setting might mean missing something crucial.
Yet, with so many alerts coming through, it can be overwhelming – and almost impossible – to sort the important information from the rest.
Why do we have popups?
Pop-ups are much like passing a sign on the road. They are meant to inform your decisions, whether this be about a hidden hazard or general navigation. In health care, they have proliferated across the increasing number of digital platforms and pieces of software health professionals use to provide patient care and nowhere more so than clinical decision-support tools.
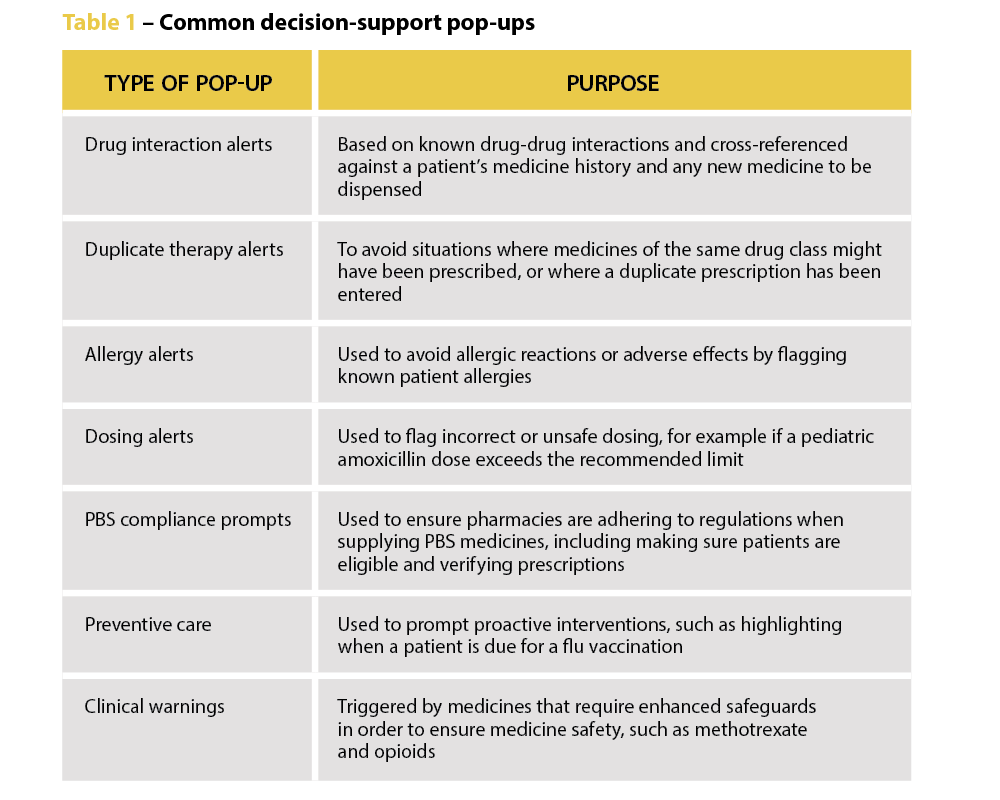
Decision-support pop-ups take many forms, from alerts about potential drug interactions to duplicate therapy warnings and allergy information. They are intended to aid health professionals in their decision-making and, in the case of dispensing pharmacists, are there to ‘remind pharmacists to be alert and to double-check that the medicine supplied is the medicine prescribed’, says PDL Senior Professional Officer Gary West FPS (he/him).
‘It might only take half a second to view them, but the difference for a patient – and for a pharmacist – can be really significant. We’ve had multiple cases where a locum or newly registered pharmacist hasn’t realised a patient is on a staged-supply arrangement because it wasn’t clear in their profile. A warning message would have prevented that patient from getting access to a larger quantity of medicines than intended.’
Mr West says both pharmacists and dispensary technicians should understand why the alerts are there – to help mitigate risk for patients and themselves.
‘We would always encourage pharmacists to use that technology, and to ensure their dispensary technicians are well trained and alert to raising certain pop-up warnings with the pharmacist associated with the dispensing event,’ says Mr West.
The pop-up paradox
But are we currently overwhelmed by pop-ups? And are some pop-ups better than others?
University of Sydney Professor of Health Research Melissa Baysari (she/her) suggests the answer to both questions is yes. A human factors expert, she has conducted extensive research into how digital health can support medicine management. Despite their good intentions, she says there is limited evidence that alerts change practice or improve patient outcomes, particularly in the hospital setting.
In a 5-year study involving patients across five hospitals in New South Wales and Queensland, Prof Baysari’s team examined whether activating drug-drug interaction alerts reduced harm. One group of hospitals had the alerts enabled, the control group did not.
Surprising results
‘We found overall that the alerts had no impact,’ she says. ‘Having drug-drug interaction alerts did not reduce the number of clinically relevant interactions or harms experienced by patients. The study shows that if you’re going to turn all the drug interaction alerts on, they’re not going to deliver the safety benefits you expect.’
In fact, she warns that poorly designed or excessive alerts can backfire. ‘There are so many negative consequences, like wasted time, frustration for clinicians and patient safety implications, that I would not recommend turning drug-drug interaction alerts on in your systems unless you’ve got some kind of smart technology in there.’
Despite the lack of evidence about the effectiveness of alerts, organisations are often reluctant to scale them back. Prof Baysari said her team had ‘a lot of trouble’ finding hospitals that were willing to not turn on their drug interaction alerts.
‘Everyone assumed the alerts were effective and they were going to be removing an intervention that was providing a safety net for everyone,’ she says. ‘But the way I see it, if organisations just keep putting more and more alerts in, it becomes the end user’s responsibility to work out which ones are relevant and act appropriately. It’s shifting the responsibility away from the organisation, so if an incident occurs, it’s the clinician who’s to blame. I think that’s very unfair.’
Information overload
Research shows that the number of alerts a healthcare professional receives impacts how effective they are – and pharmacists see a lot, Prof Baysari says.
‘You might assume that there’s an evidence base for alerts, but we have a lot more research showing that when you implement large numbers of alerts, clinicians begin to ignore them. They’re seeing too many, and so they’re not reading the recommendations. I have a theory that this becomes a habitual response – an alert pops up, clinicians override it and move past it. It allows them to get through work quickly.’
This alert fatigue has real-world safety implications. If one alert out of 12 presented is a critical warning, and the other 11 aren’t clinically relevant for the patient, it’s likely the important alert will be missed.
 ‘We’re increasingly seeing incidents where alert fatigue has been identified as a contributing factor. It’s not that there wasn’t an alert in place, but that it was lost among the other alerts the clinician saw,’ Prof Baysari says.
‘We’re increasingly seeing incidents where alert fatigue has been identified as a contributing factor. It’s not that there wasn’t an alert in place, but that it was lost among the other alerts the clinician saw,’ Prof Baysari says.
Returning to the road-sign analogy, there comes a point where there are just too many and you just can’t process them all and they stop being useful. Or you drive past the same ones every day and stop paying attention to them.
PDL has developed its own alerts based on incidents that are frequently reported to the organisation and on medicines that are more likely to have significant consequences for patients.
‘We’re very mindful. We put in a small number of pop-ups that we think are of high importance or significance,’ Mr West says. ‘Our warnings are not theoretical. We try to prevent alert fatigue by limiting warnings to things that occur with frequency or with such consequence that they justify the pop-up. We appreciate it’s difficult when hundreds of prescriptions are dispensed every day, but we’d really encourage pharmacists to take note of them and not just tab through without any consideration.’
Making smarter systems
As pharmacists continue to expand their scope of practice, Fred IT Group Partnerships Manager Regina Cowie (she/her) says the functionality of decision-support tools will need to expand to include options like preventive care recommendations and chronic disease management tools.
‘For example, clinical decision support may be used to identify patients eligible for chronic disease screening or to assess chronic disease management,’ she says. ‘Or a vaccination prompt for eligible patients could support pharmacists to make informed decisions by dynamically changing aspects within dispensing systems to guide on healthcare opportunities, for example to improve vaccination rates.’
As well as being broader, alerts also need to become smarter. Artificial intelligence is already being used in some aspects of dispensing software, Ms Cowie says, and AI has the potential to revolutionise the way clinical decision support is used.
‘AI has the ability to analyse large amounts of patient data and provide opportunities to improve medicine safety and patient care … Fred AID (Artificial Intelligence Directions) is an optional function already in place in Fred Dispense Plus. It uses AI to predict medication directions and allows pharmacists to quickly and safely enter directions for dispensing labels, rather than typing these from scratch.
‘In future, AI may suggest treatment plans or identify patients at risk of certain diseases, based on patient population data. In health care, where time pressures are a consistent burden on clinicians, a related opportunity from AI is its ability to provide administrative support by automating documentation such as clinical notes.’
Ultimately, there isn’t anything inherently wrong with alerts, Prof Baysari says, they just need to be better. ‘We have very basic alerts at the moment. They’re not designed well, so we’re not seeing the benefits. But we could.
‘We need better design in the backend, using AI to make them smarter, and, in the frontend, we need to think about how they look on screen,’ she says. ‘If we had good interfaces and a good backend infrastructure we’d get good safety benefits. But we have a lot of work to do.’
Fred IT Government and Industry Engagement Lead and former Medicines Safety Program Director of the Australian Digital Health Agency Andrew Matthews MPS says clinical decision-support tools such as alerts can increase detection of inappropriate prescribing and dispensing, improve disease management, reduce adverse patient outcomes and enhance appropriate treatment.
Fred IT, for example, has introduced an optional prompt in its dispensing software to help improve vaccination rates for the shingles vaccine in target cohorts aligned with recommendations from the National Immunisation Program (NIP).
The prompt displays only if the patient meets the NIP criteria of the patient demographics entered in the Fred Dispense Plus patient profile.
‘With the large volumes of patient data now available in electronic medical records and pharmacy systems, especially where patient disease complexity makes it difficult to quickly assess the available data,’ Mr Matthews says, ‘clinical decision-support can present relevant patient information to the clinician to facilitate clinical problem-solving, decision-making or provide additional knowledge consistent with best practice guidelines.’
[post_title] => Are pop-ups doing more harm than good?
[post_excerpt] => Are decision-support tools the problem or the cure for patient safety? Australian Pharmacist investigates.
[post_status] => publish
[comment_status] => open
[ping_status] => open
[post_password] =>
[post_name] => are-decision-support-tools-pop-ups-getting-in-the-way
[to_ping] =>
[pinged] =>
[post_modified] => 2025-06-30 15:03:26
[post_modified_gmt] => 2025-06-30 05:03:26
[post_content_filtered] =>
[post_parent] => 0
[guid] => https://www.australianpharmacist.com.au/?p=29777
[menu_order] => 0
[post_type] => post
[post_mime_type] =>
[comment_count] => 0
[filter] => raw
)
[title_attribute] => Are pop-ups doing more harm than good?
[title] => Are pop-ups doing more harm than good?
[href] => https://www.australianpharmacist.com.au/are-decision-support-tools-pop-ups-getting-in-the-way/
[module_atts:td_module:private] => Array
(
)
[td_review:protected] => Array
(
)
[is_review:protected] =>
[post_thumb_id:protected] => 29791
[authorType] =>
)

td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29766
[post_author] => 3410
[post_date] => 2025-06-25 13:10:45
[post_date_gmt] => 2025-06-25 03:10:45
[post_content] => From 1 July 2025, pharmacists will see a range of adjustments to how they deliver and bill for vaccination.
Here, Australian Pharmacist outlines the changes in vaccination services and fees pharmacists can expect from early next month.
1. NIPVIP vaccine administration fees will (slightly) increase
In 2025, the Consumer Price Index (CPI) rose by 2.4%. So from next month, there will be a CPI increase applied to all National Immunisation Program Vaccinations in Pharmacy (NIPVIP) vaccines administered. Pharmacists will receive $20.05 per vaccine administered, up from $19.60.
2. The COVID-19 vaccination payment will (significantly) drop
In less than a week, community pharmacists will see a significant reduction in the COVID-19 vaccine administration fee. The new rate will be $20.05 per vaccine administration in all Australian locations.
This is a significant decrease from the previous rates per dose, which were:

td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29757
[post_author] => 3410
[post_date] => 2025-06-23 15:11:56
[post_date_gmt] => 2025-06-23 05:11:56
[post_content] => As investigations reveal many popular high-SPF sunscreens don’t live up to their labels, both pharmacists and pharmacy assistants have a greater role to play in promoting a holistic sun protection routine.
On 12 June 2025, consumer advocacy group CHOICE released findings of a review on 20 popular SPF50 and SPF50+ brands – revealing that many don’t stack up as claimed.
According to the findings, only 20% (4) sunscreens met their SPF claims – with one Australian brand, Ultra Violette Lean Screen SPF 50+ Matifying Zinc Skinscreen, measuring only SPF 4.
Last week, the Therapeutic Goods Administration (TGA) vowed to investigate the matter.
With confidence in sunscreen already undermined via social media claims that its ingredients are toxic, how should pharmacists promote sun safety?
How do SPF numbers translate into real-world UV protection?
Australia has the highest incidence of melanoma in the world. So when the UV Index is 3 or above, it’s advisable to use a broad-spectrum, water-resistant sunscreen with an SPF30 or higher to protect against both UVA and UVB rays.
Despite the CHOICE findings, the difference in SPF ratings is not as stark as it seems. For example, Sunscreens with SPF 50 block around 98% of ultraviolet radiation (UVR), whereas SPF 30 formulations block roughly 96.7%.
So if unprotected skin begins to redden after 5 minutes in the sun, using an SPF50 formulation should, in theory, delay that reaction by fifty times – equating to roughly 250 minutes of protection. Likewise, an SPF30 product would ideally extend safe exposure to about 150 minutes. But by that rationale, an SPF4 sunscreen would only provide 20 minutes of protection – proving very limited benefit.
Application thickness also matters, Professor Rachel Neale, Senior Group Leader at the QIMR Berghofer Medical Research Institute told Australian Pharmacist.
‘The amount of sunscreen people apply will make a substantial difference to the SPF.’
What advice should pharmacists provide?
Even if the sunscreens don't meet their marketed claims, pharmacists should remind patients that they likely still offer a reasonable level of protection if used according to reapplication instructions.
Since pharmacy assistants often field questions about over-the-counter products such as sunscreen, pharmacists must ensure they’re fully across this messaging, including:

td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29266
[post_author] => 10446
[post_date] => 2025-06-20 13:53:19
[post_date_gmt] => 2025-06-20 03:53:19
[post_content] => Case scenario
Mrs Alvarez, an 82-year-old woman, presents to your pharmacy with a new prescription for apixaban 5 mg twice daily and some discharge paperwork, following a recent hospital admission after a fall at home. You notice that she was diagnosed with AF during her stay. Her medical history includes a myocardial infarction (MI) 2 years ago, for which she has been taking metoprolol, atorvastatin and aspirin.
Sponsorship statement
Funded by the Australian Government through the Quality Use of Diagnostics, Therapeutics and Pathology Program
Learning objectivesAfter reading this article, pharmacists should be able to:
|
Atrial fibrillation (AF) is the most common recurrent arrhythmia worldwide,1 characterised by uncoordinated atrial activity and irregular ventricular contractions. While its causes and contributors are many, all share a common sequela – an increased risk of ischaemic stroke that can be mitigated by anticoagulation.1 While the use of anticoagulants since the emergence of direct-acting oral anticoagulants has increased, the prevalence of AF has grown.1 This has been accompanied by a rise in hospitalisations both directly due to AF, and indirectly due to stroke and its complications.1 Pharmacists can significantly enhance AF care through direct patient engagement and collaboration with other healthcare professionals across all practice settings. Understanding key aspects of AF, its clinical features and evidence-based treatment strategies allows pharmacists to contribute positively to the overall management of individuals living with the condition.
The prevalence of AF is rising, with over 500,000 Australians estimated to have the condition in 2020,1 and over 600,000 projected by 2034.2 Although this is likely to be an underestimate of the true prevalence of AF in Australia.2
Complications arising from AF pose a substantial health burden, with a fivefold increase in the risk of stroke.3 In 2017–18 there were over 72,000 hospitalisations for AF in Australia, with the condition contributing to 9% of deaths in 2018.1 In 2015–16, AF-related healthcare expenditure in Australia was $881 million, with 69% attributed to hospital costs.1
AF results from electrophysiological abnormalities that underlie impulse generation in the heart, and/or structural irregularities that impair rapid and uniform impulse conduction.4 AF often arises from abnormal electrical activity triggered by ectopic action potentials originating in the pulmonary veins of the left atrium.4 Ongoing clinically meaningful AF requires underlying structural or electrical changes in the heart that continue to disrupt normal conduction and contraction.5 An interactive animation demonstrating cardiac activity in AF from the American Heart Association is available at https://watchlearnlive.heart.org/CVML_Mobile.php?moduleSelect=atrfib.
AF arises from a combination of genetic, metabolic, and environmental factors.4 Contributors include oxidative stress (such as alcohol intake or sleep-disordered breathing), pro-inflammatory states (diabetes and obesity), structural atrial changes (heart failure), genetics and aging.4 These conditions are interlinked, reinforcing the concept that “AF begets AF”.4 In other words, the conditions that cause AF can worsen AF, and AF can also worsen these conditions. The main sequela to this is increased stroke risk. This is caused due to the irregular contractions of the left atria leading to stasis of blood, predisposing to thrombus formation. If the thrombus embolises, it can shift into the ventricle and enter systemic circulation and subsequently the carotid arteries, leading to the embolus becoming lodged in the cerebral arteries.
 Beyond the arrhythmia, AF often signals broader pathological processes that impair cardiac function and reduce quality of life and life expectancy.5 Many of these conditions are closely linked to social determinants of health, disproportionately affecting populations with socioeconomic disadvantage. Effective AF management requires addressing both the arrhythmia and its underlying contributors.4
Beyond the arrhythmia, AF often signals broader pathological processes that impair cardiac function and reduce quality of life and life expectancy.5 Many of these conditions are closely linked to social determinants of health, disproportionately affecting populations with socioeconomic disadvantage. Effective AF management requires addressing both the arrhythmia and its underlying contributors.4
Symptoms
Like many cardiac conditions, AF symptoms can vary between individuals and overlap with other conditions, including coronary syndromes, heart failure, COPD and asthma. Common symptoms include5:
In addition, some individuals with AF may be completely asymptomatic.4
AF is also linked to higher rates of dementia and depression compared to the general population.5 Several tools are available to assess symptom burden and stratify the impact of symptoms, such as the modified European Heart Rhythm Association Score.5 Understanding the burden of AF and its associated comorbidities is essential for providing a holistic approach to patient care.
Stroke risk
The first sign of AF can be a stroke. The Australian Institute of Health and Welfare reported that in 2017–18, AF was present in 15.5% of patients hospitalised for stroke.1
Stroke risk varies, and the CHA2DS2-VA calculator is widely used in clinical practice to estimate the risk of stroke in AF.6 Points are assigned based on the following parameters7:
Scores range from 0 (ischaemic stroke incidence rate of 0.5 per 100 patient years) through to 8 (19.5 per 100 patient years).7 Scores may be used to inform decisions around initiating anticoagulation. There are other tools available, such as the GARFIELD-AF calculator, which offer more precise risk prediction, including bleeding and mortality, but require more detailed data.4
AF is diagnosed with the use of a 12-lead electrocardiogram (ECG). The ECG typically demonstrates an absence of discernible P waves and an irregularly irregular rhythm.5
Most recent international guidelines recommend further investigation for episodes lasting 30 seconds or more, with many anticoagulant trials requiring at least two separate ECGs demonstrating AF.5 Ambulatory monitors (e.g. Holter monitor) can be used for periods of 24 hours to a week and should not be confused with personal wearable devices.5
It is considered good practice to opportunistically screen for AF in patients ≥65 years of age or Aboriginal and Torres Strait Islander patients ≥50 years of age.8,9 Pharmacists may have the opportunity to do so when performing a blood pressure check, however it should be noted that automatic blood pressure machines may not always reliably detect the presence of AF.9
Wearable devices
TGA-approved wearable smart watches and devices are appropriate tools to assist in screening for AF,10 although diagnosis needs to be confirmed by an ECG that has been interpreted by a physician.5
Atrial flutter versus atrial fibrillation
Atrial flutter, a separate diagnosis to AF, is characterised as an atrial tachyarrhythmia but with regular atrial and ventricular activity. Nearly half of those diagnosed with atrial flutter will progress to atrial fibrillation.5 While stroke risk is elevated, it is not always elevated to the extent of AF.5
To address underlying causes or factors contributing to AF, tests recommended at diagnosis include5:
Further tests (e.g. for obstructive sleep apnoea and coronary artery disease) may be required for some patients to optimise management and improve outcomes.5
Treatments
The latest European Society of Cardiology (ESC) guidelines introduced the AF-CARE pathway, which emphasises treating contributing comorbidities and adopting a holistic person-centred approach to AF management.5 This replaces the previous ABC approach (Anticoagulation, Better symptom control, and Comorbidity management).5
 C – Comorbidity and risk factor management
C – Comorbidity and risk factor management
As outlined, many comorbidities increase the risk of developing AF, and contribute to increased risk of stroke (e.g. diabetes, hypertension, heart failure). Monitoring and managing these conditions is a priority in AF. Class 1 recommendations include5:
A – Avoid stroke and thromboembolism
Stroke risk assessment is important for determining anticoagulation needs. Across all guidelines there is consensus supporting anticoagulation for CHA2DS2-VA ≥2.4,5,11,12 There is less evidence for anticoagulant use in lower risk scores. In all cases, ongoing risk assessment and shared decision-making in balancing modifiable and non-modifiable risks for stroke and bleeding are key for successful management.5
R – Reduce symptoms by rate and rhythm control
Many patients with AF require interventions or treatments that control heart rate, revert to sinus rhythm or maintain sinus rhythm, leading to improved symptoms and outcomes.5 Treatment options include5:
E – Evaluation and dynamic reassessment
The ‘newest’ addition to previous treatment pathways ensures management adapts to changes in stroke risk, symptoms, comorbidities and other individual needs.5 Generally, a 6–12 monthly follow-up is recommended.5 Further guidance is available from the Quality Use of Medicines Alliance clinical guidance at https://go.medcast.com.au/anticoagulant-management-atrial-fibrillation-clinical-guide.
The role of anticoagulant therapy
AF significantly increases the risk of stroke, making timely assessment and anticoagulation critical. Oral anticoagulants reduce the risk of stroke by 64% and all-cause mortality by 26% in patients with AF.13,14
Direct-acting oral anticoagulants (DOACs)
DOACs have transformed ischaemic stroke prevention in AF (excluding patients with moderate/severe mitral stenosis or mechanical heart valves).5
Landmark trials (RE-LY, Rocket AF, and Aristotle) demonstrated their non-inferiority to warfarin in reducing the risk of stroke and systemic embolism, while halving the risk of intracranial haemorrhage.5
While DOACs offer advantages, no direct comparisons exist between apixaban, rivaroxaban and dabigatran. Choice of agent relies heavily on patient-specific factors such as age, renal function, comorbidities and bleeding risk, as well as practical considerations like accessibility and practicality of dosing regimens.
While stroke prevention benefits are well-established, prescribers must also address potential harms, including bleeding risk. Guidelines recommend addressing bleeding risk factors such as: discontinuing NSAIDs, reducing alcohol intake, lowering falls risk, and ceasing concomitant antiplatelets >12 months post-MI.4,5
However, limitations in the current DOAC evidence base warrant careful consideration. For instance, challenges remain for patients with extremes of bodyweight (BMI) above 40 kg/m² or >120 kg, where data on safety and efficacy remain sparse.4 Additionally, DOACs’ short half-lives mean anticoagulation will be compromised with any missed doses or therapy interruptions.15 Table 1 provides information on currently available oral anticoagulants.16
 Warfarin
Warfarin
While DOACs are recommended over vitamin K antagonists (VKA) to prevent ischaemic stroke and thromboembolism in AF, patients with mechanical heart valves or moderate-to-severe mitral stenosis and AF should be anticoagulated with a VKA such as warfarin.5 Pharmacists may support patients prescribed warfarin by taking time to discuss their INR target range, the importance of consistent INR recording, and by providing strategies to improve INR control.
Role of the electrophysiologists
Electrophysiologists are cardiologists specialising in arrhythmias and rhythm control procedures such as catheter ablations. They practise in both public and private settings, and are often consulted for difficult-to-treat AF. While cardiologist referral is important for follow-up and treatment escalation, it should not delay assessing risk and commencing anticoagulation or arrhythmia treatments.
Role of the GP
GPs are integral to diagnosis and commencing the initial management of AF, as well as commencing appropriate therapies and specialist referral. Importantly, comorbidity diagnosis and ongoing management are also central to the GP role.
Role of the pharmacist
Stroke and bleeding risk change over time and may be influenced by new medical conditions or medicines that increase or decrease anticoagulant activity. Pharmacists play a pivotal role in addressing these issues by providing advice on day-to-day medicine use, reducing risks such as bleeding, medicine interactions and ongoing monitoring. Like all chronic conditions, adherence to risk-reducing therapies is an ongoing challenge, and there are a range of mitigating strategies pharmacists can use.17 Pharmacists may consider offering tailored solutions to suit individual needs – this might be in the form of dose administration aids or dose reminders. Encouraging Home Medicines Reviews and supporting patients to keep an up-to-date medicines list can all encourage patients’ self-advocacy and clinicians’ decision-making. Tools like the PSA’s Quick Reference Guide can further aid pharmacists in optimising medicine use. See www.psa.org.au/career-and-support/qum/qum-alliance/oral-anticoagulants/
All patients with recent presentations for AF may be eligible for publicly funded cardiac rehabilitation, which combines education, exercise assessments and ongoing planning by a multidisciplinary team. These programs improve exercise tolerance, support weight loss and promote physical activity – all key AF management strategies.5 Many centres also offer ongoing exercise therapy or referral to tailored programs. All health professionals can refer patients, and the Heart Foundation provides an Australia-wide cardiac rehabilitation directory. Further information on these centres is available at: www.heartfoundation.org.au/your-heart/cardiac-services-directory.
Pharmacists have an essential role in providing medicines education to individuals who are prescribed anticoagulant medicines. Education should be patient-centred, culturally appropriate and include details on the importance of adherence, expected side effects and potential drug interactions. Pharmacists can offer personalised education on minimising bleeding risk by recommending reduced alcohol consumption, avoiding NSAIDs and addressing fall prevention strategies. Incorporating broader cardiovascular risk advice, like smoking cessation, weight management, and promoting blood pressure and diabetes control, may improve AF outcomes. Patients with AF can be offered further support in the form of an anticoagulation plan. A sample anticoagulation plan is available at https://go.medcast.com.au/anticoagulant-care-plan. It is essential that anticoagulants are dosed in accordance with patient characteristics. Pharmacists should flag patients who may benefit from dose adjustment based on weight, renal function or age. When appropriate, patients can be referred to their local cardiac rehabilitation centres.
Given the increasing prevalence of AF, the importance of individualised anticoagulant treatment plans cannot be overstated. Pharmacists can support early detection of AF in at-risk patients and optimise use of oral anticoagulants through medication management services, patient education and ongoing monitoring. By working collaboratively as part of the multidisciplinary team, pharmacists can significantly impact the care of patients with AF.
| Case scenario continued Prior to dispensing Mrs Alvarez her apixaban, you assess the prescribed dose. You ask her if she would mind being weighed and record her weight as 57 kg. Given her age (≥80 years) and low weight (<60 kg), you identify that she meets the criteria for a dose reduction of apixaban to 2.5 mg twice daily, regardless of her renal function. You contact the prescriber, who agrees to the dose reduction. During the conversation, you also raise your concern about the elevated bleeding risk with the concurrent use of aspirin. The prescriber confirms the intention was to discontinue aspirin before starting apixaban. You then counsel Mrs Alvarez on her updated medication regimen. You discuss the importance of adherence, signs of bleeding and stroke, and strategies for fall prevention to ensure safe and effective anticoagulation therapy. |
Adam Livori BAppSci(NucMed), BPharm(Hons), MClinPharm, FSCANZ, FAdPha, FANZCAP(Cardiol, Research) is a cardiology pharmacist and the Lead Pharmacist for Medicine and Continuing Care at Grampians Health.
Jarrah Anderson BPharm is a Clinical Lead at Medcast.
Rawa Osman MPharm, MClinTria(Res), FSHPA, FANZCAP (MedsMgmt, PublicHlth) is a Director at QUM Connect, and Research and Design Lead for the Quality Use of Medicines Alliance.
Julie Briggs MPS (she/her) B Pharm, CredPharm (MMR), FANZCAP (Generalist, PublicHlth)
Rawa Osman is currently Design Lead for the Quality Use of Medicines Alliance, which is leading a national program focused on oral anticoagulants used in AF.
[post_title] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [post_excerpt] => Atrial fibrillation is the most common recurrent arrhythmia worldwide, and can put patients at increased risk of stroke. [post_status] => publish [comment_status] => open [ping_status] => open [post_password] => [post_name] => balancing-the-scale-the-role-of-oral-anticoagulants-in-atrial-fibrillation [to_ping] => [pinged] => [post_modified] => 2025-06-25 16:14:57 [post_modified_gmt] => 2025-06-25 06:14:57 [post_content_filtered] => [post_parent] => 0 [guid] => https://www.australianpharmacist.com.au/?p=29266 [menu_order] => 0 [post_type] => post [post_mime_type] => [comment_count] => 0 [filter] => raw ) [title_attribute] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [title] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [href] => https://www.australianpharmacist.com.au/balancing-the-scale-the-role-of-oral-anticoagulants-in-atrial-fibrillation/ [module_atts:td_module:private] => Array ( ) [td_review:protected] => Array ( [td_post_template] => single_template_4 ) [is_review:protected] => [post_thumb_id:protected] => 29742 [authorType] => )td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29793
[post_author] => 3410
[post_date] => 2025-06-30 12:58:25
[post_date_gmt] => 2025-06-30 02:58:25
[post_content] => This week pharmacists will see a suite of regulatory and funding changes take effect.
Here are the six key updates pharmacists need to know before tomorrow.
1. Dispensing fees will marginally rise
Under the Eighth Community Pharmacy Agreement, pharmacists’ dispensing fee – along with the Tier 1 Administration, Handling and Infrastructure fee and the Dangerous Drug fee – will be indexed by the Consumer Price Index (CPI) annually on 1 July.
Over the past 12 months to the March 2025 quarter, the CPI increased to 2.4%.
So from tomorrow, there will be a slight jump in the per script dispense fee, which will rise from $8.67 to $8.89.
2. (Dis)continued dispensing as emergency measures roll back
As of tomorrow, temporary emergency measures that expanded the range of medicines available under Pharmaceutical Benefits Scheme (PBS) Continued Dispensing arrangements will be repealed.
The emergency authority which authorised these Continued Dispensing arrangements for private and PBS prescriptions in New South Wales, will also end at 11:59 pm tonight.
Only the standard list of 149 PBS-listed molecules will be available under Continued Dispensing in most jurisdictions, covering conditions such as asthma, diabetes, heart disease, high cholesterol and HIV.
However, Continued Dispensing will continue for some. Just enacted in Queensland, the amount of medicine a pharmacist can supply to a patient as an ‘emergency supply’ is increasing from 3 days’ supply to the smallest available manufacturer’s pack of the medicine. This applies in addition to the supply provisions enabled under the Commonwealth Continued Dispensing Determination. And in Tasmania permanent regulation also allows full Continued Dispensing as private supply for all Prescription Only Medicines.
A full list of what’s happening in your state or territory is available via PSA’s Regulation Hub which will be updated overnight to reflect these changes.
The PSA has long advocated for the full measure to be made permanent across the nation.
‘We’ve seen temporary continued dispensing measures introduced during natural disasters, which is important, but there are several scenarios where a permanent policy would help patients, from personal emergencies to natural disasters,’ said PSA CEO Adjunct Associate Professor Steve Morris.
‘PSA is again urging the federal government to work with state and territory governments to permanently protect emergency access to medicines.’
3. New vaping standards will come into effect
From 1 July, the Therapeutic Goods Administration (TGA) will implement strengthened standards for all therapeutic nicotine vaping products used for smoking-cessation and nicotine-dependence. This measure is designed to mitigate risks associated with therapeutic vaping products and ensure a consistent level of safety and quality across all products supplied through pharmacies.
Under the new standards, pharmacies will only be permitted to supply vapes that satisfy defined criteria around permitted ingredients, tamper-evident and child-resistant packaging, and clear, consistent labelling.
Pharmacists should refer to the TGA’s notified vape list, which details all therapeutic vaping products approved for smoking cessation and the management of nicotine dependence.
4. Pharmacists now have longer to transition to the new MMR and ACOP credential
Until recently, pharmacists were required to meet the revised credentialing standards by 30 June 2025 – either by obtaining Recognition of Prior Learning (RPL) towards their new credential or by undertaking further education to fulfil the updated requirements.
The deadlines to achieve both credentials have now been extended to:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29777
[post_author] => 235
[post_date] => 2025-06-27 09:36:24
[post_date_gmt] => 2025-06-26 23:36:24
[post_content] => Decision-support tools are designed to promote patient safety. But when here's a pop-up for everything, the message can be diluted.
We all know the feeling. You’re in the middle of something – maybe deep into a busy shift in the pharmacy, or on the wards in the hospital, or even scrolling on your phone at home – and another pop-up appears.
You’ve seen it before, so your instinct is to dismiss it without a second thought.
While ignoring the latest alert from your fitness app might mean falling behind on your step count, dismissing a decision-support pop-up in a healthcare setting might mean missing something crucial.
Yet, with so many alerts coming through, it can be overwhelming – and almost impossible – to sort the important information from the rest.
Why do we have popups?
Pop-ups are much like passing a sign on the road. They are meant to inform your decisions, whether this be about a hidden hazard or general navigation. In health care, they have proliferated across the increasing number of digital platforms and pieces of software health professionals use to provide patient care and nowhere more so than clinical decision-support tools.
Decision-support pop-ups take many forms, from alerts about potential drug interactions to duplicate therapy warnings and allergy information. They are intended to aid health professionals in their decision-making and, in the case of dispensing pharmacists, are there to ‘remind pharmacists to be alert and to double-check that the medicine supplied is the medicine prescribed’, says PDL Senior Professional Officer Gary West FPS (he/him).
‘It might only take half a second to view them, but the difference for a patient – and for a pharmacist – can be really significant. We’ve had multiple cases where a locum or newly registered pharmacist hasn’t realised a patient is on a staged-supply arrangement because it wasn’t clear in their profile. A warning message would have prevented that patient from getting access to a larger quantity of medicines than intended.’
Mr West says both pharmacists and dispensary technicians should understand why the alerts are there – to help mitigate risk for patients and themselves.
‘We would always encourage pharmacists to use that technology, and to ensure their dispensary technicians are well trained and alert to raising certain pop-up warnings with the pharmacist associated with the dispensing event,’ says Mr West.
The pop-up paradox
But are we currently overwhelmed by pop-ups? And are some pop-ups better than others?
University of Sydney Professor of Health Research Melissa Baysari (she/her) suggests the answer to both questions is yes. A human factors expert, she has conducted extensive research into how digital health can support medicine management. Despite their good intentions, she says there is limited evidence that alerts change practice or improve patient outcomes, particularly in the hospital setting.
In a 5-year study involving patients across five hospitals in New South Wales and Queensland, Prof Baysari’s team examined whether activating drug-drug interaction alerts reduced harm. One group of hospitals had the alerts enabled, the control group did not.
Surprising results
‘We found overall that the alerts had no impact,’ she says. ‘Having drug-drug interaction alerts did not reduce the number of clinically relevant interactions or harms experienced by patients. The study shows that if you’re going to turn all the drug interaction alerts on, they’re not going to deliver the safety benefits you expect.’
In fact, she warns that poorly designed or excessive alerts can backfire. ‘There are so many negative consequences, like wasted time, frustration for clinicians and patient safety implications, that I would not recommend turning drug-drug interaction alerts on in your systems unless you’ve got some kind of smart technology in there.’
Despite the lack of evidence about the effectiveness of alerts, organisations are often reluctant to scale them back. Prof Baysari said her team had ‘a lot of trouble’ finding hospitals that were willing to not turn on their drug interaction alerts.
‘Everyone assumed the alerts were effective and they were going to be removing an intervention that was providing a safety net for everyone,’ she says. ‘But the way I see it, if organisations just keep putting more and more alerts in, it becomes the end user’s responsibility to work out which ones are relevant and act appropriately. It’s shifting the responsibility away from the organisation, so if an incident occurs, it’s the clinician who’s to blame. I think that’s very unfair.’
Information overload
Research shows that the number of alerts a healthcare professional receives impacts how effective they are – and pharmacists see a lot, Prof Baysari says.
‘You might assume that there’s an evidence base for alerts, but we have a lot more research showing that when you implement large numbers of alerts, clinicians begin to ignore them. They’re seeing too many, and so they’re not reading the recommendations. I have a theory that this becomes a habitual response – an alert pops up, clinicians override it and move past it. It allows them to get through work quickly.’
This alert fatigue has real-world safety implications. If one alert out of 12 presented is a critical warning, and the other 11 aren’t clinically relevant for the patient, it’s likely the important alert will be missed.
‘We’re increasingly seeing incidents where alert fatigue has been identified as a contributing factor. It’s not that there wasn’t an alert in place, but that it was lost among the other alerts the clinician saw,’ Prof Baysari says.
Returning to the road-sign analogy, there comes a point where there are just too many and you just can’t process them all and they stop being useful. Or you drive past the same ones every day and stop paying attention to them.
PDL has developed its own alerts based on incidents that are frequently reported to the organisation and on medicines that are more likely to have significant consequences for patients.
‘We’re very mindful. We put in a small number of pop-ups that we think are of high importance or significance,’ Mr West says. ‘Our warnings are not theoretical. We try to prevent alert fatigue by limiting warnings to things that occur with frequency or with such consequence that they justify the pop-up. We appreciate it’s difficult when hundreds of prescriptions are dispensed every day, but we’d really encourage pharmacists to take note of them and not just tab through without any consideration.’
Making smarter systems
As pharmacists continue to expand their scope of practice, Fred IT Group Partnerships Manager Regina Cowie (she/her) says the functionality of decision-support tools will need to expand to include options like preventive care recommendations and chronic disease management tools.
‘For example, clinical decision support may be used to identify patients eligible for chronic disease screening or to assess chronic disease management,’ she says. ‘Or a vaccination prompt for eligible patients could support pharmacists to make informed decisions by dynamically changing aspects within dispensing systems to guide on healthcare opportunities, for example to improve vaccination rates.’
As well as being broader, alerts also need to become smarter. Artificial intelligence is already being used in some aspects of dispensing software, Ms Cowie says, and AI has the potential to revolutionise the way clinical decision support is used.
‘AI has the ability to analyse large amounts of patient data and provide opportunities to improve medicine safety and patient care … Fred AID (Artificial Intelligence Directions) is an optional function already in place in Fred Dispense Plus. It uses AI to predict medication directions and allows pharmacists to quickly and safely enter directions for dispensing labels, rather than typing these from scratch.
‘In future, AI may suggest treatment plans or identify patients at risk of certain diseases, based on patient population data. In health care, where time pressures are a consistent burden on clinicians, a related opportunity from AI is its ability to provide administrative support by automating documentation such as clinical notes.’
Ultimately, there isn’t anything inherently wrong with alerts, Prof Baysari says, they just need to be better. ‘We have very basic alerts at the moment. They’re not designed well, so we’re not seeing the benefits. But we could.
‘We need better design in the backend, using AI to make them smarter, and, in the frontend, we need to think about how they look on screen,’ she says. ‘If we had good interfaces and a good backend infrastructure we’d get good safety benefits. But we have a lot of work to do.’
Fred IT Government and Industry Engagement Lead and former Medicines Safety Program Director of the Australian Digital Health Agency Andrew Matthews MPS says clinical decision-support tools such as alerts can increase detection of inappropriate prescribing and dispensing, improve disease management, reduce adverse patient outcomes and enhance appropriate treatment.
Fred IT, for example, has introduced an optional prompt in its dispensing software to help improve vaccination rates for the shingles vaccine in target cohorts aligned with recommendations from the National Immunisation Program (NIP).
The prompt displays only if the patient meets the NIP criteria of the patient demographics entered in the Fred Dispense Plus patient profile.
‘With the large volumes of patient data now available in electronic medical records and pharmacy systems, especially where patient disease complexity makes it difficult to quickly assess the available data,’ Mr Matthews says, ‘clinical decision-support can present relevant patient information to the clinician to facilitate clinical problem-solving, decision-making or provide additional knowledge consistent with best practice guidelines.’
[post_title] => Are pop-ups doing more harm than good?
[post_excerpt] => Are decision-support tools the problem or the cure for patient safety? Australian Pharmacist investigates.
[post_status] => publish
[comment_status] => open
[ping_status] => open
[post_password] =>
[post_name] => are-decision-support-tools-pop-ups-getting-in-the-way
[to_ping] =>
[pinged] =>
[post_modified] => 2025-06-30 15:03:26
[post_modified_gmt] => 2025-06-30 05:03:26
[post_content_filtered] =>
[post_parent] => 0
[guid] => https://www.australianpharmacist.com.au/?p=29777
[menu_order] => 0
[post_type] => post
[post_mime_type] =>
[comment_count] => 0
[filter] => raw
)
[title_attribute] => Are pop-ups doing more harm than good?
[title] => Are pop-ups doing more harm than good?
[href] => https://www.australianpharmacist.com.au/are-decision-support-tools-pop-ups-getting-in-the-way/
[module_atts:td_module:private] => Array
(
)
[td_review:protected] => Array
(
)
[is_review:protected] =>
[post_thumb_id:protected] => 29791
[authorType] =>
)
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29766
[post_author] => 3410
[post_date] => 2025-06-25 13:10:45
[post_date_gmt] => 2025-06-25 03:10:45
[post_content] => From 1 July 2025, pharmacists will see a range of adjustments to how they deliver and bill for vaccination.
Here, Australian Pharmacist outlines the changes in vaccination services and fees pharmacists can expect from early next month.
1. NIPVIP vaccine administration fees will (slightly) increase
In 2025, the Consumer Price Index (CPI) rose by 2.4%. So from next month, there will be a CPI increase applied to all National Immunisation Program Vaccinations in Pharmacy (NIPVIP) vaccines administered. Pharmacists will receive $20.05 per vaccine administered, up from $19.60.
2. The COVID-19 vaccination payment will (significantly) drop
In less than a week, community pharmacists will see a significant reduction in the COVID-19 vaccine administration fee. The new rate will be $20.05 per vaccine administration in all Australian locations.
This is a significant decrease from the previous rates per dose, which were:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29757
[post_author] => 3410
[post_date] => 2025-06-23 15:11:56
[post_date_gmt] => 2025-06-23 05:11:56
[post_content] => As investigations reveal many popular high-SPF sunscreens don’t live up to their labels, both pharmacists and pharmacy assistants have a greater role to play in promoting a holistic sun protection routine.
On 12 June 2025, consumer advocacy group CHOICE released findings of a review on 20 popular SPF50 and SPF50+ brands – revealing that many don’t stack up as claimed.
According to the findings, only 20% (4) sunscreens met their SPF claims – with one Australian brand, Ultra Violette Lean Screen SPF 50+ Matifying Zinc Skinscreen, measuring only SPF 4.
Last week, the Therapeutic Goods Administration (TGA) vowed to investigate the matter.
With confidence in sunscreen already undermined via social media claims that its ingredients are toxic, how should pharmacists promote sun safety?
How do SPF numbers translate into real-world UV protection?
Australia has the highest incidence of melanoma in the world. So when the UV Index is 3 or above, it’s advisable to use a broad-spectrum, water-resistant sunscreen with an SPF30 or higher to protect against both UVA and UVB rays.
Despite the CHOICE findings, the difference in SPF ratings is not as stark as it seems. For example, Sunscreens with SPF 50 block around 98% of ultraviolet radiation (UVR), whereas SPF 30 formulations block roughly 96.7%.
So if unprotected skin begins to redden after 5 minutes in the sun, using an SPF50 formulation should, in theory, delay that reaction by fifty times – equating to roughly 250 minutes of protection. Likewise, an SPF30 product would ideally extend safe exposure to about 150 minutes. But by that rationale, an SPF4 sunscreen would only provide 20 minutes of protection – proving very limited benefit.
Application thickness also matters, Professor Rachel Neale, Senior Group Leader at the QIMR Berghofer Medical Research Institute told Australian Pharmacist.
‘The amount of sunscreen people apply will make a substantial difference to the SPF.’
What advice should pharmacists provide?
Even if the sunscreens don't meet their marketed claims, pharmacists should remind patients that they likely still offer a reasonable level of protection if used according to reapplication instructions.
Since pharmacy assistants often field questions about over-the-counter products such as sunscreen, pharmacists must ensure they’re fully across this messaging, including:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29266
[post_author] => 10446
[post_date] => 2025-06-20 13:53:19
[post_date_gmt] => 2025-06-20 03:53:19
[post_content] => Case scenario
Mrs Alvarez, an 82-year-old woman, presents to your pharmacy with a new prescription for apixaban 5 mg twice daily and some discharge paperwork, following a recent hospital admission after a fall at home. You notice that she was diagnosed with AF during her stay. Her medical history includes a myocardial infarction (MI) 2 years ago, for which she has been taking metoprolol, atorvastatin and aspirin.
Sponsorship statement
Funded by the Australian Government through the Quality Use of Diagnostics, Therapeutics and Pathology Program
Learning objectivesAfter reading this article, pharmacists should be able to:
|
Atrial fibrillation (AF) is the most common recurrent arrhythmia worldwide,1 characterised by uncoordinated atrial activity and irregular ventricular contractions. While its causes and contributors are many, all share a common sequela – an increased risk of ischaemic stroke that can be mitigated by anticoagulation.1 While the use of anticoagulants since the emergence of direct-acting oral anticoagulants has increased, the prevalence of AF has grown.1 This has been accompanied by a rise in hospitalisations both directly due to AF, and indirectly due to stroke and its complications.1 Pharmacists can significantly enhance AF care through direct patient engagement and collaboration with other healthcare professionals across all practice settings. Understanding key aspects of AF, its clinical features and evidence-based treatment strategies allows pharmacists to contribute positively to the overall management of individuals living with the condition.
The prevalence of AF is rising, with over 500,000 Australians estimated to have the condition in 2020,1 and over 600,000 projected by 2034.2 Although this is likely to be an underestimate of the true prevalence of AF in Australia.2
Complications arising from AF pose a substantial health burden, with a fivefold increase in the risk of stroke.3 In 2017–18 there were over 72,000 hospitalisations for AF in Australia, with the condition contributing to 9% of deaths in 2018.1 In 2015–16, AF-related healthcare expenditure in Australia was $881 million, with 69% attributed to hospital costs.1
AF results from electrophysiological abnormalities that underlie impulse generation in the heart, and/or structural irregularities that impair rapid and uniform impulse conduction.4 AF often arises from abnormal electrical activity triggered by ectopic action potentials originating in the pulmonary veins of the left atrium.4 Ongoing clinically meaningful AF requires underlying structural or electrical changes in the heart that continue to disrupt normal conduction and contraction.5 An interactive animation demonstrating cardiac activity in AF from the American Heart Association is available at https://watchlearnlive.heart.org/CVML_Mobile.php?moduleSelect=atrfib.
AF arises from a combination of genetic, metabolic, and environmental factors.4 Contributors include oxidative stress (such as alcohol intake or sleep-disordered breathing), pro-inflammatory states (diabetes and obesity), structural atrial changes (heart failure), genetics and aging.4 These conditions are interlinked, reinforcing the concept that “AF begets AF”.4 In other words, the conditions that cause AF can worsen AF, and AF can also worsen these conditions. The main sequela to this is increased stroke risk. This is caused due to the irregular contractions of the left atria leading to stasis of blood, predisposing to thrombus formation. If the thrombus embolises, it can shift into the ventricle and enter systemic circulation and subsequently the carotid arteries, leading to the embolus becoming lodged in the cerebral arteries.
Beyond the arrhythmia, AF often signals broader pathological processes that impair cardiac function and reduce quality of life and life expectancy.5 Many of these conditions are closely linked to social determinants of health, disproportionately affecting populations with socioeconomic disadvantage. Effective AF management requires addressing both the arrhythmia and its underlying contributors.4
Symptoms
Like many cardiac conditions, AF symptoms can vary between individuals and overlap with other conditions, including coronary syndromes, heart failure, COPD and asthma. Common symptoms include5:
In addition, some individuals with AF may be completely asymptomatic.4
AF is also linked to higher rates of dementia and depression compared to the general population.5 Several tools are available to assess symptom burden and stratify the impact of symptoms, such as the modified European Heart Rhythm Association Score.5 Understanding the burden of AF and its associated comorbidities is essential for providing a holistic approach to patient care.
Stroke risk
The first sign of AF can be a stroke. The Australian Institute of Health and Welfare reported that in 2017–18, AF was present in 15.5% of patients hospitalised for stroke.1
Stroke risk varies, and the CHA2DS2-VA calculator is widely used in clinical practice to estimate the risk of stroke in AF.6 Points are assigned based on the following parameters7:
Scores range from 0 (ischaemic stroke incidence rate of 0.5 per 100 patient years) through to 8 (19.5 per 100 patient years).7 Scores may be used to inform decisions around initiating anticoagulation. There are other tools available, such as the GARFIELD-AF calculator, which offer more precise risk prediction, including bleeding and mortality, but require more detailed data.4
AF is diagnosed with the use of a 12-lead electrocardiogram (ECG). The ECG typically demonstrates an absence of discernible P waves and an irregularly irregular rhythm.5
Most recent international guidelines recommend further investigation for episodes lasting 30 seconds or more, with many anticoagulant trials requiring at least two separate ECGs demonstrating AF.5 Ambulatory monitors (e.g. Holter monitor) can be used for periods of 24 hours to a week and should not be confused with personal wearable devices.5
It is considered good practice to opportunistically screen for AF in patients ≥65 years of age or Aboriginal and Torres Strait Islander patients ≥50 years of age.8,9 Pharmacists may have the opportunity to do so when performing a blood pressure check, however it should be noted that automatic blood pressure machines may not always reliably detect the presence of AF.9
Wearable devices
TGA-approved wearable smart watches and devices are appropriate tools to assist in screening for AF,10 although diagnosis needs to be confirmed by an ECG that has been interpreted by a physician.5
Atrial flutter versus atrial fibrillation
Atrial flutter, a separate diagnosis to AF, is characterised as an atrial tachyarrhythmia but with regular atrial and ventricular activity. Nearly half of those diagnosed with atrial flutter will progress to atrial fibrillation.5 While stroke risk is elevated, it is not always elevated to the extent of AF.5
To address underlying causes or factors contributing to AF, tests recommended at diagnosis include5:
Further tests (e.g. for obstructive sleep apnoea and coronary artery disease) may be required for some patients to optimise management and improve outcomes.5
Treatments
The latest European Society of Cardiology (ESC) guidelines introduced the AF-CARE pathway, which emphasises treating contributing comorbidities and adopting a holistic person-centred approach to AF management.5 This replaces the previous ABC approach (Anticoagulation, Better symptom control, and Comorbidity management).5
C – Comorbidity and risk factor management
As outlined, many comorbidities increase the risk of developing AF, and contribute to increased risk of stroke (e.g. diabetes, hypertension, heart failure). Monitoring and managing these conditions is a priority in AF. Class 1 recommendations include5:
A – Avoid stroke and thromboembolism
Stroke risk assessment is important for determining anticoagulation needs. Across all guidelines there is consensus supporting anticoagulation for CHA2DS2-VA ≥2.4,5,11,12 There is less evidence for anticoagulant use in lower risk scores. In all cases, ongoing risk assessment and shared decision-making in balancing modifiable and non-modifiable risks for stroke and bleeding are key for successful management.5
R – Reduce symptoms by rate and rhythm control
Many patients with AF require interventions or treatments that control heart rate, revert to sinus rhythm or maintain sinus rhythm, leading to improved symptoms and outcomes.5 Treatment options include5:
E – Evaluation and dynamic reassessment
The ‘newest’ addition to previous treatment pathways ensures management adapts to changes in stroke risk, symptoms, comorbidities and other individual needs.5 Generally, a 6–12 monthly follow-up is recommended.5 Further guidance is available from the Quality Use of Medicines Alliance clinical guidance at https://go.medcast.com.au/anticoagulant-management-atrial-fibrillation-clinical-guide.
The role of anticoagulant therapy
AF significantly increases the risk of stroke, making timely assessment and anticoagulation critical. Oral anticoagulants reduce the risk of stroke by 64% and all-cause mortality by 26% in patients with AF.13,14
Direct-acting oral anticoagulants (DOACs)
DOACs have transformed ischaemic stroke prevention in AF (excluding patients with moderate/severe mitral stenosis or mechanical heart valves).5
Landmark trials (RE-LY, Rocket AF, and Aristotle) demonstrated their non-inferiority to warfarin in reducing the risk of stroke and systemic embolism, while halving the risk of intracranial haemorrhage.5
While DOACs offer advantages, no direct comparisons exist between apixaban, rivaroxaban and dabigatran. Choice of agent relies heavily on patient-specific factors such as age, renal function, comorbidities and bleeding risk, as well as practical considerations like accessibility and practicality of dosing regimens.
While stroke prevention benefits are well-established, prescribers must also address potential harms, including bleeding risk. Guidelines recommend addressing bleeding risk factors such as: discontinuing NSAIDs, reducing alcohol intake, lowering falls risk, and ceasing concomitant antiplatelets >12 months post-MI.4,5
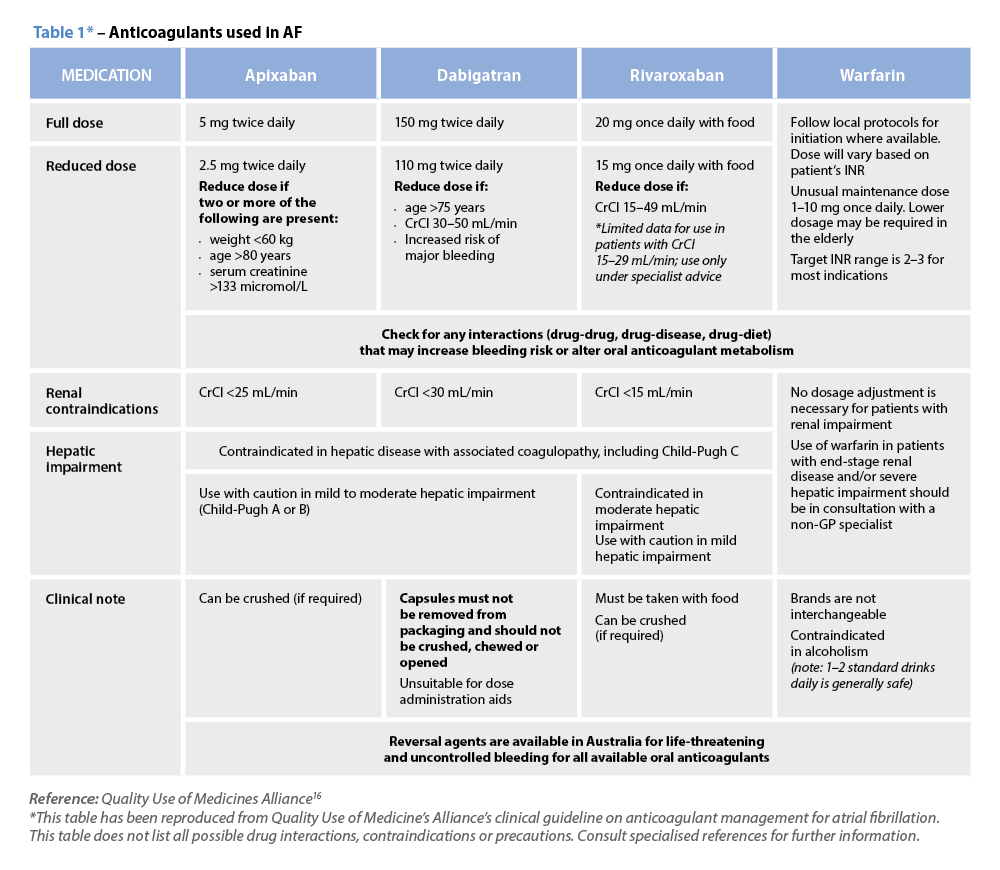
However, limitations in the current DOAC evidence base warrant careful consideration. For instance, challenges remain for patients with extremes of bodyweight (BMI) above 40 kg/m² or >120 kg, where data on safety and efficacy remain sparse.4 Additionally, DOACs’ short half-lives mean anticoagulation will be compromised with any missed doses or therapy interruptions.15 Table 1 provides information on currently available oral anticoagulants.16
Warfarin
While DOACs are recommended over vitamin K antagonists (VKA) to prevent ischaemic stroke and thromboembolism in AF, patients with mechanical heart valves or moderate-to-severe mitral stenosis and AF should be anticoagulated with a VKA such as warfarin.5 Pharmacists may support patients prescribed warfarin by taking time to discuss their INR target range, the importance of consistent INR recording, and by providing strategies to improve INR control.
Role of the electrophysiologists
Electrophysiologists are cardiologists specialising in arrhythmias and rhythm control procedures such as catheter ablations. They practise in both public and private settings, and are often consulted for difficult-to-treat AF. While cardiologist referral is important for follow-up and treatment escalation, it should not delay assessing risk and commencing anticoagulation or arrhythmia treatments.
Role of the GP
GPs are integral to diagnosis and commencing the initial management of AF, as well as commencing appropriate therapies and specialist referral. Importantly, comorbidity diagnosis and ongoing management are also central to the GP role.
Role of the pharmacist
Stroke and bleeding risk change over time and may be influenced by new medical conditions or medicines that increase or decrease anticoagulant activity. Pharmacists play a pivotal role in addressing these issues by providing advice on day-to-day medicine use, reducing risks such as bleeding, medicine interactions and ongoing monitoring. Like all chronic conditions, adherence to risk-reducing therapies is an ongoing challenge, and there are a range of mitigating strategies pharmacists can use.17 Pharmacists may consider offering tailored solutions to suit individual needs – this might be in the form of dose administration aids or dose reminders. Encouraging Home Medicines Reviews and supporting patients to keep an up-to-date medicines list can all encourage patients’ self-advocacy and clinicians’ decision-making. Tools like the PSA’s Quick Reference Guide can further aid pharmacists in optimising medicine use. See www.psa.org.au/career-and-support/qum/qum-alliance/oral-anticoagulants/
All patients with recent presentations for AF may be eligible for publicly funded cardiac rehabilitation, which combines education, exercise assessments and ongoing planning by a multidisciplinary team. These programs improve exercise tolerance, support weight loss and promote physical activity – all key AF management strategies.5 Many centres also offer ongoing exercise therapy or referral to tailored programs. All health professionals can refer patients, and the Heart Foundation provides an Australia-wide cardiac rehabilitation directory. Further information on these centres is available at: www.heartfoundation.org.au/your-heart/cardiac-services-directory.
Pharmacists have an essential role in providing medicines education to individuals who are prescribed anticoagulant medicines. Education should be patient-centred, culturally appropriate and include details on the importance of adherence, expected side effects and potential drug interactions. Pharmacists can offer personalised education on minimising bleeding risk by recommending reduced alcohol consumption, avoiding NSAIDs and addressing fall prevention strategies. Incorporating broader cardiovascular risk advice, like smoking cessation, weight management, and promoting blood pressure and diabetes control, may improve AF outcomes. Patients with AF can be offered further support in the form of an anticoagulation plan. A sample anticoagulation plan is available at https://go.medcast.com.au/anticoagulant-care-plan. It is essential that anticoagulants are dosed in accordance with patient characteristics. Pharmacists should flag patients who may benefit from dose adjustment based on weight, renal function or age. When appropriate, patients can be referred to their local cardiac rehabilitation centres.
Given the increasing prevalence of AF, the importance of individualised anticoagulant treatment plans cannot be overstated. Pharmacists can support early detection of AF in at-risk patients and optimise use of oral anticoagulants through medication management services, patient education and ongoing monitoring. By working collaboratively as part of the multidisciplinary team, pharmacists can significantly impact the care of patients with AF.
| Case scenario continued Prior to dispensing Mrs Alvarez her apixaban, you assess the prescribed dose. You ask her if she would mind being weighed and record her weight as 57 kg. Given her age (≥80 years) and low weight (<60 kg), you identify that she meets the criteria for a dose reduction of apixaban to 2.5 mg twice daily, regardless of her renal function. You contact the prescriber, who agrees to the dose reduction. During the conversation, you also raise your concern about the elevated bleeding risk with the concurrent use of aspirin. The prescriber confirms the intention was to discontinue aspirin before starting apixaban. You then counsel Mrs Alvarez on her updated medication regimen. You discuss the importance of adherence, signs of bleeding and stroke, and strategies for fall prevention to ensure safe and effective anticoagulation therapy. |
Adam Livori BAppSci(NucMed), BPharm(Hons), MClinPharm, FSCANZ, FAdPha, FANZCAP(Cardiol, Research) is a cardiology pharmacist and the Lead Pharmacist for Medicine and Continuing Care at Grampians Health.
Jarrah Anderson BPharm is a Clinical Lead at Medcast.
Rawa Osman MPharm, MClinTria(Res), FSHPA, FANZCAP (MedsMgmt, PublicHlth) is a Director at QUM Connect, and Research and Design Lead for the Quality Use of Medicines Alliance.
Julie Briggs MPS (she/her) B Pharm, CredPharm (MMR), FANZCAP (Generalist, PublicHlth)
Rawa Osman is currently Design Lead for the Quality Use of Medicines Alliance, which is leading a national program focused on oral anticoagulants used in AF.
[post_title] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [post_excerpt] => Atrial fibrillation is the most common recurrent arrhythmia worldwide, and can put patients at increased risk of stroke. [post_status] => publish [comment_status] => open [ping_status] => open [post_password] => [post_name] => balancing-the-scale-the-role-of-oral-anticoagulants-in-atrial-fibrillation [to_ping] => [pinged] => [post_modified] => 2025-06-25 16:14:57 [post_modified_gmt] => 2025-06-25 06:14:57 [post_content_filtered] => [post_parent] => 0 [guid] => https://www.australianpharmacist.com.au/?p=29266 [menu_order] => 0 [post_type] => post [post_mime_type] => [comment_count] => 0 [filter] => raw ) [title_attribute] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [title] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [href] => https://www.australianpharmacist.com.au/balancing-the-scale-the-role-of-oral-anticoagulants-in-atrial-fibrillation/ [module_atts:td_module:private] => Array ( ) [td_review:protected] => Array ( [td_post_template] => single_template_4 ) [is_review:protected] => [post_thumb_id:protected] => 29742 [authorType] => )td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29793
[post_author] => 3410
[post_date] => 2025-06-30 12:58:25
[post_date_gmt] => 2025-06-30 02:58:25
[post_content] => This week pharmacists will see a suite of regulatory and funding changes take effect.
Here are the six key updates pharmacists need to know before tomorrow.
1. Dispensing fees will marginally rise
Under the Eighth Community Pharmacy Agreement, pharmacists’ dispensing fee – along with the Tier 1 Administration, Handling and Infrastructure fee and the Dangerous Drug fee – will be indexed by the Consumer Price Index (CPI) annually on 1 July.
Over the past 12 months to the March 2025 quarter, the CPI increased to 2.4%.
So from tomorrow, there will be a slight jump in the per script dispense fee, which will rise from $8.67 to $8.89.
2. (Dis)continued dispensing as emergency measures roll back
As of tomorrow, temporary emergency measures that expanded the range of medicines available under Pharmaceutical Benefits Scheme (PBS) Continued Dispensing arrangements will be repealed.
The emergency authority which authorised these Continued Dispensing arrangements for private and PBS prescriptions in New South Wales, will also end at 11:59 pm tonight.
Only the standard list of 149 PBS-listed molecules will be available under Continued Dispensing in most jurisdictions, covering conditions such as asthma, diabetes, heart disease, high cholesterol and HIV.
However, Continued Dispensing will continue for some. Just enacted in Queensland, the amount of medicine a pharmacist can supply to a patient as an ‘emergency supply’ is increasing from 3 days’ supply to the smallest available manufacturer’s pack of the medicine. This applies in addition to the supply provisions enabled under the Commonwealth Continued Dispensing Determination. And in Tasmania permanent regulation also allows full Continued Dispensing as private supply for all Prescription Only Medicines.
A full list of what’s happening in your state or territory is available via PSA’s Regulation Hub which will be updated overnight to reflect these changes.
The PSA has long advocated for the full measure to be made permanent across the nation.
‘We’ve seen temporary continued dispensing measures introduced during natural disasters, which is important, but there are several scenarios where a permanent policy would help patients, from personal emergencies to natural disasters,’ said PSA CEO Adjunct Associate Professor Steve Morris.
‘PSA is again urging the federal government to work with state and territory governments to permanently protect emergency access to medicines.’
3. New vaping standards will come into effect
From 1 July, the Therapeutic Goods Administration (TGA) will implement strengthened standards for all therapeutic nicotine vaping products used for smoking-cessation and nicotine-dependence. This measure is designed to mitigate risks associated with therapeutic vaping products and ensure a consistent level of safety and quality across all products supplied through pharmacies.
Under the new standards, pharmacies will only be permitted to supply vapes that satisfy defined criteria around permitted ingredients, tamper-evident and child-resistant packaging, and clear, consistent labelling.
Pharmacists should refer to the TGA’s notified vape list, which details all therapeutic vaping products approved for smoking cessation and the management of nicotine dependence.
4. Pharmacists now have longer to transition to the new MMR and ACOP credential
Until recently, pharmacists were required to meet the revised credentialing standards by 30 June 2025 – either by obtaining Recognition of Prior Learning (RPL) towards their new credential or by undertaking further education to fulfil the updated requirements.
The deadlines to achieve both credentials have now been extended to:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29777
[post_author] => 235
[post_date] => 2025-06-27 09:36:24
[post_date_gmt] => 2025-06-26 23:36:24
[post_content] => Decision-support tools are designed to promote patient safety. But when here's a pop-up for everything, the message can be diluted.
We all know the feeling. You’re in the middle of something – maybe deep into a busy shift in the pharmacy, or on the wards in the hospital, or even scrolling on your phone at home – and another pop-up appears.
You’ve seen it before, so your instinct is to dismiss it without a second thought.
While ignoring the latest alert from your fitness app might mean falling behind on your step count, dismissing a decision-support pop-up in a healthcare setting might mean missing something crucial.
Yet, with so many alerts coming through, it can be overwhelming – and almost impossible – to sort the important information from the rest.
Why do we have popups?
Pop-ups are much like passing a sign on the road. They are meant to inform your decisions, whether this be about a hidden hazard or general navigation. In health care, they have proliferated across the increasing number of digital platforms and pieces of software health professionals use to provide patient care and nowhere more so than clinical decision-support tools.
Decision-support pop-ups take many forms, from alerts about potential drug interactions to duplicate therapy warnings and allergy information. They are intended to aid health professionals in their decision-making and, in the case of dispensing pharmacists, are there to ‘remind pharmacists to be alert and to double-check that the medicine supplied is the medicine prescribed’, says PDL Senior Professional Officer Gary West FPS (he/him).
‘It might only take half a second to view them, but the difference for a patient – and for a pharmacist – can be really significant. We’ve had multiple cases where a locum or newly registered pharmacist hasn’t realised a patient is on a staged-supply arrangement because it wasn’t clear in their profile. A warning message would have prevented that patient from getting access to a larger quantity of medicines than intended.’
Mr West says both pharmacists and dispensary technicians should understand why the alerts are there – to help mitigate risk for patients and themselves.
‘We would always encourage pharmacists to use that technology, and to ensure their dispensary technicians are well trained and alert to raising certain pop-up warnings with the pharmacist associated with the dispensing event,’ says Mr West.
The pop-up paradox
But are we currently overwhelmed by pop-ups? And are some pop-ups better than others?
University of Sydney Professor of Health Research Melissa Baysari (she/her) suggests the answer to both questions is yes. A human factors expert, she has conducted extensive research into how digital health can support medicine management. Despite their good intentions, she says there is limited evidence that alerts change practice or improve patient outcomes, particularly in the hospital setting.
In a 5-year study involving patients across five hospitals in New South Wales and Queensland, Prof Baysari’s team examined whether activating drug-drug interaction alerts reduced harm. One group of hospitals had the alerts enabled, the control group did not.
Surprising results
‘We found overall that the alerts had no impact,’ she says. ‘Having drug-drug interaction alerts did not reduce the number of clinically relevant interactions or harms experienced by patients. The study shows that if you’re going to turn all the drug interaction alerts on, they’re not going to deliver the safety benefits you expect.’
In fact, she warns that poorly designed or excessive alerts can backfire. ‘There are so many negative consequences, like wasted time, frustration for clinicians and patient safety implications, that I would not recommend turning drug-drug interaction alerts on in your systems unless you’ve got some kind of smart technology in there.’
Despite the lack of evidence about the effectiveness of alerts, organisations are often reluctant to scale them back. Prof Baysari said her team had ‘a lot of trouble’ finding hospitals that were willing to not turn on their drug interaction alerts.
‘Everyone assumed the alerts were effective and they were going to be removing an intervention that was providing a safety net for everyone,’ she says. ‘But the way I see it, if organisations just keep putting more and more alerts in, it becomes the end user’s responsibility to work out which ones are relevant and act appropriately. It’s shifting the responsibility away from the organisation, so if an incident occurs, it’s the clinician who’s to blame. I think that’s very unfair.’
Information overload
Research shows that the number of alerts a healthcare professional receives impacts how effective they are – and pharmacists see a lot, Prof Baysari says.
‘You might assume that there’s an evidence base for alerts, but we have a lot more research showing that when you implement large numbers of alerts, clinicians begin to ignore them. They’re seeing too many, and so they’re not reading the recommendations. I have a theory that this becomes a habitual response – an alert pops up, clinicians override it and move past it. It allows them to get through work quickly.’
This alert fatigue has real-world safety implications. If one alert out of 12 presented is a critical warning, and the other 11 aren’t clinically relevant for the patient, it’s likely the important alert will be missed.
‘We’re increasingly seeing incidents where alert fatigue has been identified as a contributing factor. It’s not that there wasn’t an alert in place, but that it was lost among the other alerts the clinician saw,’ Prof Baysari says.
Returning to the road-sign analogy, there comes a point where there are just too many and you just can’t process them all and they stop being useful. Or you drive past the same ones every day and stop paying attention to them.
PDL has developed its own alerts based on incidents that are frequently reported to the organisation and on medicines that are more likely to have significant consequences for patients.
‘We’re very mindful. We put in a small number of pop-ups that we think are of high importance or significance,’ Mr West says. ‘Our warnings are not theoretical. We try to prevent alert fatigue by limiting warnings to things that occur with frequency or with such consequence that they justify the pop-up. We appreciate it’s difficult when hundreds of prescriptions are dispensed every day, but we’d really encourage pharmacists to take note of them and not just tab through without any consideration.’
Making smarter systems
As pharmacists continue to expand their scope of practice, Fred IT Group Partnerships Manager Regina Cowie (she/her) says the functionality of decision-support tools will need to expand to include options like preventive care recommendations and chronic disease management tools.
‘For example, clinical decision support may be used to identify patients eligible for chronic disease screening or to assess chronic disease management,’ she says. ‘Or a vaccination prompt for eligible patients could support pharmacists to make informed decisions by dynamically changing aspects within dispensing systems to guide on healthcare opportunities, for example to improve vaccination rates.’
As well as being broader, alerts also need to become smarter. Artificial intelligence is already being used in some aspects of dispensing software, Ms Cowie says, and AI has the potential to revolutionise the way clinical decision support is used.
‘AI has the ability to analyse large amounts of patient data and provide opportunities to improve medicine safety and patient care … Fred AID (Artificial Intelligence Directions) is an optional function already in place in Fred Dispense Plus. It uses AI to predict medication directions and allows pharmacists to quickly and safely enter directions for dispensing labels, rather than typing these from scratch.
‘In future, AI may suggest treatment plans or identify patients at risk of certain diseases, based on patient population data. In health care, where time pressures are a consistent burden on clinicians, a related opportunity from AI is its ability to provide administrative support by automating documentation such as clinical notes.’
Ultimately, there isn’t anything inherently wrong with alerts, Prof Baysari says, they just need to be better. ‘We have very basic alerts at the moment. They’re not designed well, so we’re not seeing the benefits. But we could.
‘We need better design in the backend, using AI to make them smarter, and, in the frontend, we need to think about how they look on screen,’ she says. ‘If we had good interfaces and a good backend infrastructure we’d get good safety benefits. But we have a lot of work to do.’
Fred IT Government and Industry Engagement Lead and former Medicines Safety Program Director of the Australian Digital Health Agency Andrew Matthews MPS says clinical decision-support tools such as alerts can increase detection of inappropriate prescribing and dispensing, improve disease management, reduce adverse patient outcomes and enhance appropriate treatment.
Fred IT, for example, has introduced an optional prompt in its dispensing software to help improve vaccination rates for the shingles vaccine in target cohorts aligned with recommendations from the National Immunisation Program (NIP).
The prompt displays only if the patient meets the NIP criteria of the patient demographics entered in the Fred Dispense Plus patient profile.
‘With the large volumes of patient data now available in electronic medical records and pharmacy systems, especially where patient disease complexity makes it difficult to quickly assess the available data,’ Mr Matthews says, ‘clinical decision-support can present relevant patient information to the clinician to facilitate clinical problem-solving, decision-making or provide additional knowledge consistent with best practice guidelines.’
[post_title] => Are pop-ups doing more harm than good?
[post_excerpt] => Are decision-support tools the problem or the cure for patient safety? Australian Pharmacist investigates.
[post_status] => publish
[comment_status] => open
[ping_status] => open
[post_password] =>
[post_name] => are-decision-support-tools-pop-ups-getting-in-the-way
[to_ping] =>
[pinged] =>
[post_modified] => 2025-06-30 15:03:26
[post_modified_gmt] => 2025-06-30 05:03:26
[post_content_filtered] =>
[post_parent] => 0
[guid] => https://www.australianpharmacist.com.au/?p=29777
[menu_order] => 0
[post_type] => post
[post_mime_type] =>
[comment_count] => 0
[filter] => raw
)
[title_attribute] => Are pop-ups doing more harm than good?
[title] => Are pop-ups doing more harm than good?
[href] => https://www.australianpharmacist.com.au/are-decision-support-tools-pop-ups-getting-in-the-way/
[module_atts:td_module:private] => Array
(
)
[td_review:protected] => Array
(
)
[is_review:protected] =>
[post_thumb_id:protected] => 29791
[authorType] =>
)
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29766
[post_author] => 3410
[post_date] => 2025-06-25 13:10:45
[post_date_gmt] => 2025-06-25 03:10:45
[post_content] => From 1 July 2025, pharmacists will see a range of adjustments to how they deliver and bill for vaccination.
Here, Australian Pharmacist outlines the changes in vaccination services and fees pharmacists can expect from early next month.
1. NIPVIP vaccine administration fees will (slightly) increase
In 2025, the Consumer Price Index (CPI) rose by 2.4%. So from next month, there will be a CPI increase applied to all National Immunisation Program Vaccinations in Pharmacy (NIPVIP) vaccines administered. Pharmacists will receive $20.05 per vaccine administered, up from $19.60.
2. The COVID-19 vaccination payment will (significantly) drop
In less than a week, community pharmacists will see a significant reduction in the COVID-19 vaccine administration fee. The new rate will be $20.05 per vaccine administration in all Australian locations.
This is a significant decrease from the previous rates per dose, which were:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29757
[post_author] => 3410
[post_date] => 2025-06-23 15:11:56
[post_date_gmt] => 2025-06-23 05:11:56
[post_content] => As investigations reveal many popular high-SPF sunscreens don’t live up to their labels, both pharmacists and pharmacy assistants have a greater role to play in promoting a holistic sun protection routine.
On 12 June 2025, consumer advocacy group CHOICE released findings of a review on 20 popular SPF50 and SPF50+ brands – revealing that many don’t stack up as claimed.
According to the findings, only 20% (4) sunscreens met their SPF claims – with one Australian brand, Ultra Violette Lean Screen SPF 50+ Matifying Zinc Skinscreen, measuring only SPF 4.
Last week, the Therapeutic Goods Administration (TGA) vowed to investigate the matter.
With confidence in sunscreen already undermined via social media claims that its ingredients are toxic, how should pharmacists promote sun safety?
How do SPF numbers translate into real-world UV protection?
Australia has the highest incidence of melanoma in the world. So when the UV Index is 3 or above, it’s advisable to use a broad-spectrum, water-resistant sunscreen with an SPF30 or higher to protect against both UVA and UVB rays.
Despite the CHOICE findings, the difference in SPF ratings is not as stark as it seems. For example, Sunscreens with SPF 50 block around 98% of ultraviolet radiation (UVR), whereas SPF 30 formulations block roughly 96.7%.
So if unprotected skin begins to redden after 5 minutes in the sun, using an SPF50 formulation should, in theory, delay that reaction by fifty times – equating to roughly 250 minutes of protection. Likewise, an SPF30 product would ideally extend safe exposure to about 150 minutes. But by that rationale, an SPF4 sunscreen would only provide 20 minutes of protection – proving very limited benefit.
Application thickness also matters, Professor Rachel Neale, Senior Group Leader at the QIMR Berghofer Medical Research Institute told Australian Pharmacist.
‘The amount of sunscreen people apply will make a substantial difference to the SPF.’
What advice should pharmacists provide?
Even if the sunscreens don't meet their marketed claims, pharmacists should remind patients that they likely still offer a reasonable level of protection if used according to reapplication instructions.
Since pharmacy assistants often field questions about over-the-counter products such as sunscreen, pharmacists must ensure they’re fully across this messaging, including:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29266
[post_author] => 10446
[post_date] => 2025-06-20 13:53:19
[post_date_gmt] => 2025-06-20 03:53:19
[post_content] => Case scenario
Mrs Alvarez, an 82-year-old woman, presents to your pharmacy with a new prescription for apixaban 5 mg twice daily and some discharge paperwork, following a recent hospital admission after a fall at home. You notice that she was diagnosed with AF during her stay. Her medical history includes a myocardial infarction (MI) 2 years ago, for which she has been taking metoprolol, atorvastatin and aspirin.
Sponsorship statement
Funded by the Australian Government through the Quality Use of Diagnostics, Therapeutics and Pathology Program
Learning objectivesAfter reading this article, pharmacists should be able to:
|
Atrial fibrillation (AF) is the most common recurrent arrhythmia worldwide,1 characterised by uncoordinated atrial activity and irregular ventricular contractions. While its causes and contributors are many, all share a common sequela – an increased risk of ischaemic stroke that can be mitigated by anticoagulation.1 While the use of anticoagulants since the emergence of direct-acting oral anticoagulants has increased, the prevalence of AF has grown.1 This has been accompanied by a rise in hospitalisations both directly due to AF, and indirectly due to stroke and its complications.1 Pharmacists can significantly enhance AF care through direct patient engagement and collaboration with other healthcare professionals across all practice settings. Understanding key aspects of AF, its clinical features and evidence-based treatment strategies allows pharmacists to contribute positively to the overall management of individuals living with the condition.
The prevalence of AF is rising, with over 500,000 Australians estimated to have the condition in 2020,1 and over 600,000 projected by 2034.2 Although this is likely to be an underestimate of the true prevalence of AF in Australia.2
Complications arising from AF pose a substantial health burden, with a fivefold increase in the risk of stroke.3 In 2017–18 there were over 72,000 hospitalisations for AF in Australia, with the condition contributing to 9% of deaths in 2018.1 In 2015–16, AF-related healthcare expenditure in Australia was $881 million, with 69% attributed to hospital costs.1
AF results from electrophysiological abnormalities that underlie impulse generation in the heart, and/or structural irregularities that impair rapid and uniform impulse conduction.4 AF often arises from abnormal electrical activity triggered by ectopic action potentials originating in the pulmonary veins of the left atrium.4 Ongoing clinically meaningful AF requires underlying structural or electrical changes in the heart that continue to disrupt normal conduction and contraction.5 An interactive animation demonstrating cardiac activity in AF from the American Heart Association is available at https://watchlearnlive.heart.org/CVML_Mobile.php?moduleSelect=atrfib.
AF arises from a combination of genetic, metabolic, and environmental factors.4 Contributors include oxidative stress (such as alcohol intake or sleep-disordered breathing), pro-inflammatory states (diabetes and obesity), structural atrial changes (heart failure), genetics and aging.4 These conditions are interlinked, reinforcing the concept that “AF begets AF”.4 In other words, the conditions that cause AF can worsen AF, and AF can also worsen these conditions. The main sequela to this is increased stroke risk. This is caused due to the irregular contractions of the left atria leading to stasis of blood, predisposing to thrombus formation. If the thrombus embolises, it can shift into the ventricle and enter systemic circulation and subsequently the carotid arteries, leading to the embolus becoming lodged in the cerebral arteries.
Beyond the arrhythmia, AF often signals broader pathological processes that impair cardiac function and reduce quality of life and life expectancy.5 Many of these conditions are closely linked to social determinants of health, disproportionately affecting populations with socioeconomic disadvantage. Effective AF management requires addressing both the arrhythmia and its underlying contributors.4
Symptoms
Like many cardiac conditions, AF symptoms can vary between individuals and overlap with other conditions, including coronary syndromes, heart failure, COPD and asthma. Common symptoms include5:
In addition, some individuals with AF may be completely asymptomatic.4
AF is also linked to higher rates of dementia and depression compared to the general population.5 Several tools are available to assess symptom burden and stratify the impact of symptoms, such as the modified European Heart Rhythm Association Score.5 Understanding the burden of AF and its associated comorbidities is essential for providing a holistic approach to patient care.
Stroke risk
The first sign of AF can be a stroke. The Australian Institute of Health and Welfare reported that in 2017–18, AF was present in 15.5% of patients hospitalised for stroke.1
Stroke risk varies, and the CHA2DS2-VA calculator is widely used in clinical practice to estimate the risk of stroke in AF.6 Points are assigned based on the following parameters7:
Scores range from 0 (ischaemic stroke incidence rate of 0.5 per 100 patient years) through to 8 (19.5 per 100 patient years).7 Scores may be used to inform decisions around initiating anticoagulation. There are other tools available, such as the GARFIELD-AF calculator, which offer more precise risk prediction, including bleeding and mortality, but require more detailed data.4
AF is diagnosed with the use of a 12-lead electrocardiogram (ECG). The ECG typically demonstrates an absence of discernible P waves and an irregularly irregular rhythm.5
Most recent international guidelines recommend further investigation for episodes lasting 30 seconds or more, with many anticoagulant trials requiring at least two separate ECGs demonstrating AF.5 Ambulatory monitors (e.g. Holter monitor) can be used for periods of 24 hours to a week and should not be confused with personal wearable devices.5
It is considered good practice to opportunistically screen for AF in patients ≥65 years of age or Aboriginal and Torres Strait Islander patients ≥50 years of age.8,9 Pharmacists may have the opportunity to do so when performing a blood pressure check, however it should be noted that automatic blood pressure machines may not always reliably detect the presence of AF.9
Wearable devices
TGA-approved wearable smart watches and devices are appropriate tools to assist in screening for AF,10 although diagnosis needs to be confirmed by an ECG that has been interpreted by a physician.5
Atrial flutter versus atrial fibrillation
Atrial flutter, a separate diagnosis to AF, is characterised as an atrial tachyarrhythmia but with regular atrial and ventricular activity. Nearly half of those diagnosed with atrial flutter will progress to atrial fibrillation.5 While stroke risk is elevated, it is not always elevated to the extent of AF.5
To address underlying causes or factors contributing to AF, tests recommended at diagnosis include5:
Further tests (e.g. for obstructive sleep apnoea and coronary artery disease) may be required for some patients to optimise management and improve outcomes.5
Treatments
The latest European Society of Cardiology (ESC) guidelines introduced the AF-CARE pathway, which emphasises treating contributing comorbidities and adopting a holistic person-centred approach to AF management.5 This replaces the previous ABC approach (Anticoagulation, Better symptom control, and Comorbidity management).5
C – Comorbidity and risk factor management
As outlined, many comorbidities increase the risk of developing AF, and contribute to increased risk of stroke (e.g. diabetes, hypertension, heart failure). Monitoring and managing these conditions is a priority in AF. Class 1 recommendations include5:
A – Avoid stroke and thromboembolism
Stroke risk assessment is important for determining anticoagulation needs. Across all guidelines there is consensus supporting anticoagulation for CHA2DS2-VA ≥2.4,5,11,12 There is less evidence for anticoagulant use in lower risk scores. In all cases, ongoing risk assessment and shared decision-making in balancing modifiable and non-modifiable risks for stroke and bleeding are key for successful management.5
R – Reduce symptoms by rate and rhythm control
Many patients with AF require interventions or treatments that control heart rate, revert to sinus rhythm or maintain sinus rhythm, leading to improved symptoms and outcomes.5 Treatment options include5:
E – Evaluation and dynamic reassessment
The ‘newest’ addition to previous treatment pathways ensures management adapts to changes in stroke risk, symptoms, comorbidities and other individual needs.5 Generally, a 6–12 monthly follow-up is recommended.5 Further guidance is available from the Quality Use of Medicines Alliance clinical guidance at https://go.medcast.com.au/anticoagulant-management-atrial-fibrillation-clinical-guide.
The role of anticoagulant therapy
AF significantly increases the risk of stroke, making timely assessment and anticoagulation critical. Oral anticoagulants reduce the risk of stroke by 64% and all-cause mortality by 26% in patients with AF.13,14
Direct-acting oral anticoagulants (DOACs)
DOACs have transformed ischaemic stroke prevention in AF (excluding patients with moderate/severe mitral stenosis or mechanical heart valves).5
Landmark trials (RE-LY, Rocket AF, and Aristotle) demonstrated their non-inferiority to warfarin in reducing the risk of stroke and systemic embolism, while halving the risk of intracranial haemorrhage.5
While DOACs offer advantages, no direct comparisons exist between apixaban, rivaroxaban and dabigatran. Choice of agent relies heavily on patient-specific factors such as age, renal function, comorbidities and bleeding risk, as well as practical considerations like accessibility and practicality of dosing regimens.
While stroke prevention benefits are well-established, prescribers must also address potential harms, including bleeding risk. Guidelines recommend addressing bleeding risk factors such as: discontinuing NSAIDs, reducing alcohol intake, lowering falls risk, and ceasing concomitant antiplatelets >12 months post-MI.4,5
However, limitations in the current DOAC evidence base warrant careful consideration. For instance, challenges remain for patients with extremes of bodyweight (BMI) above 40 kg/m² or >120 kg, where data on safety and efficacy remain sparse.4 Additionally, DOACs’ short half-lives mean anticoagulation will be compromised with any missed doses or therapy interruptions.15 Table 1 provides information on currently available oral anticoagulants.16
Warfarin
While DOACs are recommended over vitamin K antagonists (VKA) to prevent ischaemic stroke and thromboembolism in AF, patients with mechanical heart valves or moderate-to-severe mitral stenosis and AF should be anticoagulated with a VKA such as warfarin.5 Pharmacists may support patients prescribed warfarin by taking time to discuss their INR target range, the importance of consistent INR recording, and by providing strategies to improve INR control.
Role of the electrophysiologists
Electrophysiologists are cardiologists specialising in arrhythmias and rhythm control procedures such as catheter ablations. They practise in both public and private settings, and are often consulted for difficult-to-treat AF. While cardiologist referral is important for follow-up and treatment escalation, it should not delay assessing risk and commencing anticoagulation or arrhythmia treatments.
Role of the GP
GPs are integral to diagnosis and commencing the initial management of AF, as well as commencing appropriate therapies and specialist referral. Importantly, comorbidity diagnosis and ongoing management are also central to the GP role.
Role of the pharmacist
Stroke and bleeding risk change over time and may be influenced by new medical conditions or medicines that increase or decrease anticoagulant activity. Pharmacists play a pivotal role in addressing these issues by providing advice on day-to-day medicine use, reducing risks such as bleeding, medicine interactions and ongoing monitoring. Like all chronic conditions, adherence to risk-reducing therapies is an ongoing challenge, and there are a range of mitigating strategies pharmacists can use.17 Pharmacists may consider offering tailored solutions to suit individual needs – this might be in the form of dose administration aids or dose reminders. Encouraging Home Medicines Reviews and supporting patients to keep an up-to-date medicines list can all encourage patients’ self-advocacy and clinicians’ decision-making. Tools like the PSA’s Quick Reference Guide can further aid pharmacists in optimising medicine use. See www.psa.org.au/career-and-support/qum/qum-alliance/oral-anticoagulants/
All patients with recent presentations for AF may be eligible for publicly funded cardiac rehabilitation, which combines education, exercise assessments and ongoing planning by a multidisciplinary team. These programs improve exercise tolerance, support weight loss and promote physical activity – all key AF management strategies.5 Many centres also offer ongoing exercise therapy or referral to tailored programs. All health professionals can refer patients, and the Heart Foundation provides an Australia-wide cardiac rehabilitation directory. Further information on these centres is available at: www.heartfoundation.org.au/your-heart/cardiac-services-directory.
Pharmacists have an essential role in providing medicines education to individuals who are prescribed anticoagulant medicines. Education should be patient-centred, culturally appropriate and include details on the importance of adherence, expected side effects and potential drug interactions. Pharmacists can offer personalised education on minimising bleeding risk by recommending reduced alcohol consumption, avoiding NSAIDs and addressing fall prevention strategies. Incorporating broader cardiovascular risk advice, like smoking cessation, weight management, and promoting blood pressure and diabetes control, may improve AF outcomes. Patients with AF can be offered further support in the form of an anticoagulation plan. A sample anticoagulation plan is available at https://go.medcast.com.au/anticoagulant-care-plan. It is essential that anticoagulants are dosed in accordance with patient characteristics. Pharmacists should flag patients who may benefit from dose adjustment based on weight, renal function or age. When appropriate, patients can be referred to their local cardiac rehabilitation centres.
Given the increasing prevalence of AF, the importance of individualised anticoagulant treatment plans cannot be overstated. Pharmacists can support early detection of AF in at-risk patients and optimise use of oral anticoagulants through medication management services, patient education and ongoing monitoring. By working collaboratively as part of the multidisciplinary team, pharmacists can significantly impact the care of patients with AF.
| Case scenario continued Prior to dispensing Mrs Alvarez her apixaban, you assess the prescribed dose. You ask her if she would mind being weighed and record her weight as 57 kg. Given her age (≥80 years) and low weight (<60 kg), you identify that she meets the criteria for a dose reduction of apixaban to 2.5 mg twice daily, regardless of her renal function. You contact the prescriber, who agrees to the dose reduction. During the conversation, you also raise your concern about the elevated bleeding risk with the concurrent use of aspirin. The prescriber confirms the intention was to discontinue aspirin before starting apixaban. You then counsel Mrs Alvarez on her updated medication regimen. You discuss the importance of adherence, signs of bleeding and stroke, and strategies for fall prevention to ensure safe and effective anticoagulation therapy. |
Adam Livori BAppSci(NucMed), BPharm(Hons), MClinPharm, FSCANZ, FAdPha, FANZCAP(Cardiol, Research) is a cardiology pharmacist and the Lead Pharmacist for Medicine and Continuing Care at Grampians Health.
Jarrah Anderson BPharm is a Clinical Lead at Medcast.
Rawa Osman MPharm, MClinTria(Res), FSHPA, FANZCAP (MedsMgmt, PublicHlth) is a Director at QUM Connect, and Research and Design Lead for the Quality Use of Medicines Alliance.
Julie Briggs MPS (she/her) B Pharm, CredPharm (MMR), FANZCAP (Generalist, PublicHlth)
Rawa Osman is currently Design Lead for the Quality Use of Medicines Alliance, which is leading a national program focused on oral anticoagulants used in AF.
[post_title] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [post_excerpt] => Atrial fibrillation is the most common recurrent arrhythmia worldwide, and can put patients at increased risk of stroke. [post_status] => publish [comment_status] => open [ping_status] => open [post_password] => [post_name] => balancing-the-scale-the-role-of-oral-anticoagulants-in-atrial-fibrillation [to_ping] => [pinged] => [post_modified] => 2025-06-25 16:14:57 [post_modified_gmt] => 2025-06-25 06:14:57 [post_content_filtered] => [post_parent] => 0 [guid] => https://www.australianpharmacist.com.au/?p=29266 [menu_order] => 0 [post_type] => post [post_mime_type] => [comment_count] => 0 [filter] => raw ) [title_attribute] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [title] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [href] => https://www.australianpharmacist.com.au/balancing-the-scale-the-role-of-oral-anticoagulants-in-atrial-fibrillation/ [module_atts:td_module:private] => Array ( ) [td_review:protected] => Array ( [td_post_template] => single_template_4 ) [is_review:protected] => [post_thumb_id:protected] => 29742 [authorType] => )td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29793
[post_author] => 3410
[post_date] => 2025-06-30 12:58:25
[post_date_gmt] => 2025-06-30 02:58:25
[post_content] => This week pharmacists will see a suite of regulatory and funding changes take effect.
Here are the six key updates pharmacists need to know before tomorrow.
1. Dispensing fees will marginally rise
Under the Eighth Community Pharmacy Agreement, pharmacists’ dispensing fee – along with the Tier 1 Administration, Handling and Infrastructure fee and the Dangerous Drug fee – will be indexed by the Consumer Price Index (CPI) annually on 1 July.
Over the past 12 months to the March 2025 quarter, the CPI increased to 2.4%.
So from tomorrow, there will be a slight jump in the per script dispense fee, which will rise from $8.67 to $8.89.
2. (Dis)continued dispensing as emergency measures roll back
As of tomorrow, temporary emergency measures that expanded the range of medicines available under Pharmaceutical Benefits Scheme (PBS) Continued Dispensing arrangements will be repealed.
The emergency authority which authorised these Continued Dispensing arrangements for private and PBS prescriptions in New South Wales, will also end at 11:59 pm tonight.
Only the standard list of 149 PBS-listed molecules will be available under Continued Dispensing in most jurisdictions, covering conditions such as asthma, diabetes, heart disease, high cholesterol and HIV.
However, Continued Dispensing will continue for some. Just enacted in Queensland, the amount of medicine a pharmacist can supply to a patient as an ‘emergency supply’ is increasing from 3 days’ supply to the smallest available manufacturer’s pack of the medicine. This applies in addition to the supply provisions enabled under the Commonwealth Continued Dispensing Determination. And in Tasmania permanent regulation also allows full Continued Dispensing as private supply for all Prescription Only Medicines.
A full list of what’s happening in your state or territory is available via PSA’s Regulation Hub which will be updated overnight to reflect these changes.
The PSA has long advocated for the full measure to be made permanent across the nation.
‘We’ve seen temporary continued dispensing measures introduced during natural disasters, which is important, but there are several scenarios where a permanent policy would help patients, from personal emergencies to natural disasters,’ said PSA CEO Adjunct Associate Professor Steve Morris.
‘PSA is again urging the federal government to work with state and territory governments to permanently protect emergency access to medicines.’
3. New vaping standards will come into effect
From 1 July, the Therapeutic Goods Administration (TGA) will implement strengthened standards for all therapeutic nicotine vaping products used for smoking-cessation and nicotine-dependence. This measure is designed to mitigate risks associated with therapeutic vaping products and ensure a consistent level of safety and quality across all products supplied through pharmacies.
Under the new standards, pharmacies will only be permitted to supply vapes that satisfy defined criteria around permitted ingredients, tamper-evident and child-resistant packaging, and clear, consistent labelling.
Pharmacists should refer to the TGA’s notified vape list, which details all therapeutic vaping products approved for smoking cessation and the management of nicotine dependence.
4. Pharmacists now have longer to transition to the new MMR and ACOP credential
Until recently, pharmacists were required to meet the revised credentialing standards by 30 June 2025 – either by obtaining Recognition of Prior Learning (RPL) towards their new credential or by undertaking further education to fulfil the updated requirements.
The deadlines to achieve both credentials have now been extended to:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29777
[post_author] => 235
[post_date] => 2025-06-27 09:36:24
[post_date_gmt] => 2025-06-26 23:36:24
[post_content] => Decision-support tools are designed to promote patient safety. But when here's a pop-up for everything, the message can be diluted.
We all know the feeling. You’re in the middle of something – maybe deep into a busy shift in the pharmacy, or on the wards in the hospital, or even scrolling on your phone at home – and another pop-up appears.
You’ve seen it before, so your instinct is to dismiss it without a second thought.
While ignoring the latest alert from your fitness app might mean falling behind on your step count, dismissing a decision-support pop-up in a healthcare setting might mean missing something crucial.
Yet, with so many alerts coming through, it can be overwhelming – and almost impossible – to sort the important information from the rest.
Why do we have popups?
Pop-ups are much like passing a sign on the road. They are meant to inform your decisions, whether this be about a hidden hazard or general navigation. In health care, they have proliferated across the increasing number of digital platforms and pieces of software health professionals use to provide patient care and nowhere more so than clinical decision-support tools.
Decision-support pop-ups take many forms, from alerts about potential drug interactions to duplicate therapy warnings and allergy information. They are intended to aid health professionals in their decision-making and, in the case of dispensing pharmacists, are there to ‘remind pharmacists to be alert and to double-check that the medicine supplied is the medicine prescribed’, says PDL Senior Professional Officer Gary West FPS (he/him).
‘It might only take half a second to view them, but the difference for a patient – and for a pharmacist – can be really significant. We’ve had multiple cases where a locum or newly registered pharmacist hasn’t realised a patient is on a staged-supply arrangement because it wasn’t clear in their profile. A warning message would have prevented that patient from getting access to a larger quantity of medicines than intended.’
Mr West says both pharmacists and dispensary technicians should understand why the alerts are there – to help mitigate risk for patients and themselves.
‘We would always encourage pharmacists to use that technology, and to ensure their dispensary technicians are well trained and alert to raising certain pop-up warnings with the pharmacist associated with the dispensing event,’ says Mr West.
The pop-up paradox
But are we currently overwhelmed by pop-ups? And are some pop-ups better than others?
University of Sydney Professor of Health Research Melissa Baysari (she/her) suggests the answer to both questions is yes. A human factors expert, she has conducted extensive research into how digital health can support medicine management. Despite their good intentions, she says there is limited evidence that alerts change practice or improve patient outcomes, particularly in the hospital setting.
In a 5-year study involving patients across five hospitals in New South Wales and Queensland, Prof Baysari’s team examined whether activating drug-drug interaction alerts reduced harm. One group of hospitals had the alerts enabled, the control group did not.
Surprising results
‘We found overall that the alerts had no impact,’ she says. ‘Having drug-drug interaction alerts did not reduce the number of clinically relevant interactions or harms experienced by patients. The study shows that if you’re going to turn all the drug interaction alerts on, they’re not going to deliver the safety benefits you expect.’
In fact, she warns that poorly designed or excessive alerts can backfire. ‘There are so many negative consequences, like wasted time, frustration for clinicians and patient safety implications, that I would not recommend turning drug-drug interaction alerts on in your systems unless you’ve got some kind of smart technology in there.’
Despite the lack of evidence about the effectiveness of alerts, organisations are often reluctant to scale them back. Prof Baysari said her team had ‘a lot of trouble’ finding hospitals that were willing to not turn on their drug interaction alerts.
‘Everyone assumed the alerts were effective and they were going to be removing an intervention that was providing a safety net for everyone,’ she says. ‘But the way I see it, if organisations just keep putting more and more alerts in, it becomes the end user’s responsibility to work out which ones are relevant and act appropriately. It’s shifting the responsibility away from the organisation, so if an incident occurs, it’s the clinician who’s to blame. I think that’s very unfair.’
Information overload
Research shows that the number of alerts a healthcare professional receives impacts how effective they are – and pharmacists see a lot, Prof Baysari says.
‘You might assume that there’s an evidence base for alerts, but we have a lot more research showing that when you implement large numbers of alerts, clinicians begin to ignore them. They’re seeing too many, and so they’re not reading the recommendations. I have a theory that this becomes a habitual response – an alert pops up, clinicians override it and move past it. It allows them to get through work quickly.’
This alert fatigue has real-world safety implications. If one alert out of 12 presented is a critical warning, and the other 11 aren’t clinically relevant for the patient, it’s likely the important alert will be missed.
‘We’re increasingly seeing incidents where alert fatigue has been identified as a contributing factor. It’s not that there wasn’t an alert in place, but that it was lost among the other alerts the clinician saw,’ Prof Baysari says.
Returning to the road-sign analogy, there comes a point where there are just too many and you just can’t process them all and they stop being useful. Or you drive past the same ones every day and stop paying attention to them.
PDL has developed its own alerts based on incidents that are frequently reported to the organisation and on medicines that are more likely to have significant consequences for patients.
‘We’re very mindful. We put in a small number of pop-ups that we think are of high importance or significance,’ Mr West says. ‘Our warnings are not theoretical. We try to prevent alert fatigue by limiting warnings to things that occur with frequency or with such consequence that they justify the pop-up. We appreciate it’s difficult when hundreds of prescriptions are dispensed every day, but we’d really encourage pharmacists to take note of them and not just tab through without any consideration.’
Making smarter systems
As pharmacists continue to expand their scope of practice, Fred IT Group Partnerships Manager Regina Cowie (she/her) says the functionality of decision-support tools will need to expand to include options like preventive care recommendations and chronic disease management tools.
‘For example, clinical decision support may be used to identify patients eligible for chronic disease screening or to assess chronic disease management,’ she says. ‘Or a vaccination prompt for eligible patients could support pharmacists to make informed decisions by dynamically changing aspects within dispensing systems to guide on healthcare opportunities, for example to improve vaccination rates.’
As well as being broader, alerts also need to become smarter. Artificial intelligence is already being used in some aspects of dispensing software, Ms Cowie says, and AI has the potential to revolutionise the way clinical decision support is used.
‘AI has the ability to analyse large amounts of patient data and provide opportunities to improve medicine safety and patient care … Fred AID (Artificial Intelligence Directions) is an optional function already in place in Fred Dispense Plus. It uses AI to predict medication directions and allows pharmacists to quickly and safely enter directions for dispensing labels, rather than typing these from scratch.
‘In future, AI may suggest treatment plans or identify patients at risk of certain diseases, based on patient population data. In health care, where time pressures are a consistent burden on clinicians, a related opportunity from AI is its ability to provide administrative support by automating documentation such as clinical notes.’
Ultimately, there isn’t anything inherently wrong with alerts, Prof Baysari says, they just need to be better. ‘We have very basic alerts at the moment. They’re not designed well, so we’re not seeing the benefits. But we could.
‘We need better design in the backend, using AI to make them smarter, and, in the frontend, we need to think about how they look on screen,’ she says. ‘If we had good interfaces and a good backend infrastructure we’d get good safety benefits. But we have a lot of work to do.’
Fred IT Government and Industry Engagement Lead and former Medicines Safety Program Director of the Australian Digital Health Agency Andrew Matthews MPS says clinical decision-support tools such as alerts can increase detection of inappropriate prescribing and dispensing, improve disease management, reduce adverse patient outcomes and enhance appropriate treatment.
Fred IT, for example, has introduced an optional prompt in its dispensing software to help improve vaccination rates for the shingles vaccine in target cohorts aligned with recommendations from the National Immunisation Program (NIP).
The prompt displays only if the patient meets the NIP criteria of the patient demographics entered in the Fred Dispense Plus patient profile.
‘With the large volumes of patient data now available in electronic medical records and pharmacy systems, especially where patient disease complexity makes it difficult to quickly assess the available data,’ Mr Matthews says, ‘clinical decision-support can present relevant patient information to the clinician to facilitate clinical problem-solving, decision-making or provide additional knowledge consistent with best practice guidelines.’
[post_title] => Are pop-ups doing more harm than good?
[post_excerpt] => Are decision-support tools the problem or the cure for patient safety? Australian Pharmacist investigates.
[post_status] => publish
[comment_status] => open
[ping_status] => open
[post_password] =>
[post_name] => are-decision-support-tools-pop-ups-getting-in-the-way
[to_ping] =>
[pinged] =>
[post_modified] => 2025-06-30 15:03:26
[post_modified_gmt] => 2025-06-30 05:03:26
[post_content_filtered] =>
[post_parent] => 0
[guid] => https://www.australianpharmacist.com.au/?p=29777
[menu_order] => 0
[post_type] => post
[post_mime_type] =>
[comment_count] => 0
[filter] => raw
)
[title_attribute] => Are pop-ups doing more harm than good?
[title] => Are pop-ups doing more harm than good?
[href] => https://www.australianpharmacist.com.au/are-decision-support-tools-pop-ups-getting-in-the-way/
[module_atts:td_module:private] => Array
(
)
[td_review:protected] => Array
(
)
[is_review:protected] =>
[post_thumb_id:protected] => 29791
[authorType] =>
)
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29766
[post_author] => 3410
[post_date] => 2025-06-25 13:10:45
[post_date_gmt] => 2025-06-25 03:10:45
[post_content] => From 1 July 2025, pharmacists will see a range of adjustments to how they deliver and bill for vaccination.
Here, Australian Pharmacist outlines the changes in vaccination services and fees pharmacists can expect from early next month.
1. NIPVIP vaccine administration fees will (slightly) increase
In 2025, the Consumer Price Index (CPI) rose by 2.4%. So from next month, there will be a CPI increase applied to all National Immunisation Program Vaccinations in Pharmacy (NIPVIP) vaccines administered. Pharmacists will receive $20.05 per vaccine administered, up from $19.60.
2. The COVID-19 vaccination payment will (significantly) drop
In less than a week, community pharmacists will see a significant reduction in the COVID-19 vaccine administration fee. The new rate will be $20.05 per vaccine administration in all Australian locations.
This is a significant decrease from the previous rates per dose, which were:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29757
[post_author] => 3410
[post_date] => 2025-06-23 15:11:56
[post_date_gmt] => 2025-06-23 05:11:56
[post_content] => As investigations reveal many popular high-SPF sunscreens don’t live up to their labels, both pharmacists and pharmacy assistants have a greater role to play in promoting a holistic sun protection routine.
On 12 June 2025, consumer advocacy group CHOICE released findings of a review on 20 popular SPF50 and SPF50+ brands – revealing that many don’t stack up as claimed.
According to the findings, only 20% (4) sunscreens met their SPF claims – with one Australian brand, Ultra Violette Lean Screen SPF 50+ Matifying Zinc Skinscreen, measuring only SPF 4.
Last week, the Therapeutic Goods Administration (TGA) vowed to investigate the matter.
With confidence in sunscreen already undermined via social media claims that its ingredients are toxic, how should pharmacists promote sun safety?
How do SPF numbers translate into real-world UV protection?
Australia has the highest incidence of melanoma in the world. So when the UV Index is 3 or above, it’s advisable to use a broad-spectrum, water-resistant sunscreen with an SPF30 or higher to protect against both UVA and UVB rays.
Despite the CHOICE findings, the difference in SPF ratings is not as stark as it seems. For example, Sunscreens with SPF 50 block around 98% of ultraviolet radiation (UVR), whereas SPF 30 formulations block roughly 96.7%.
So if unprotected skin begins to redden after 5 minutes in the sun, using an SPF50 formulation should, in theory, delay that reaction by fifty times – equating to roughly 250 minutes of protection. Likewise, an SPF30 product would ideally extend safe exposure to about 150 minutes. But by that rationale, an SPF4 sunscreen would only provide 20 minutes of protection – proving very limited benefit.
Application thickness also matters, Professor Rachel Neale, Senior Group Leader at the QIMR Berghofer Medical Research Institute told Australian Pharmacist.
‘The amount of sunscreen people apply will make a substantial difference to the SPF.’
What advice should pharmacists provide?
Even if the sunscreens don't meet their marketed claims, pharmacists should remind patients that they likely still offer a reasonable level of protection if used according to reapplication instructions.
Since pharmacy assistants often field questions about over-the-counter products such as sunscreen, pharmacists must ensure they’re fully across this messaging, including:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 29266
[post_author] => 10446
[post_date] => 2025-06-20 13:53:19
[post_date_gmt] => 2025-06-20 03:53:19
[post_content] => Case scenario
Mrs Alvarez, an 82-year-old woman, presents to your pharmacy with a new prescription for apixaban 5 mg twice daily and some discharge paperwork, following a recent hospital admission after a fall at home. You notice that she was diagnosed with AF during her stay. Her medical history includes a myocardial infarction (MI) 2 years ago, for which she has been taking metoprolol, atorvastatin and aspirin.
Sponsorship statement
Funded by the Australian Government through the Quality Use of Diagnostics, Therapeutics and Pathology Program
Learning objectivesAfter reading this article, pharmacists should be able to:
|
Atrial fibrillation (AF) is the most common recurrent arrhythmia worldwide,1 characterised by uncoordinated atrial activity and irregular ventricular contractions. While its causes and contributors are many, all share a common sequela – an increased risk of ischaemic stroke that can be mitigated by anticoagulation.1 While the use of anticoagulants since the emergence of direct-acting oral anticoagulants has increased, the prevalence of AF has grown.1 This has been accompanied by a rise in hospitalisations both directly due to AF, and indirectly due to stroke and its complications.1 Pharmacists can significantly enhance AF care through direct patient engagement and collaboration with other healthcare professionals across all practice settings. Understanding key aspects of AF, its clinical features and evidence-based treatment strategies allows pharmacists to contribute positively to the overall management of individuals living with the condition.
The prevalence of AF is rising, with over 500,000 Australians estimated to have the condition in 2020,1 and over 600,000 projected by 2034.2 Although this is likely to be an underestimate of the true prevalence of AF in Australia.2
Complications arising from AF pose a substantial health burden, with a fivefold increase in the risk of stroke.3 In 2017–18 there were over 72,000 hospitalisations for AF in Australia, with the condition contributing to 9% of deaths in 2018.1 In 2015–16, AF-related healthcare expenditure in Australia was $881 million, with 69% attributed to hospital costs.1
AF results from electrophysiological abnormalities that underlie impulse generation in the heart, and/or structural irregularities that impair rapid and uniform impulse conduction.4 AF often arises from abnormal electrical activity triggered by ectopic action potentials originating in the pulmonary veins of the left atrium.4 Ongoing clinically meaningful AF requires underlying structural or electrical changes in the heart that continue to disrupt normal conduction and contraction.5 An interactive animation demonstrating cardiac activity in AF from the American Heart Association is available at https://watchlearnlive.heart.org/CVML_Mobile.php?moduleSelect=atrfib.
AF arises from a combination of genetic, metabolic, and environmental factors.4 Contributors include oxidative stress (such as alcohol intake or sleep-disordered breathing), pro-inflammatory states (diabetes and obesity), structural atrial changes (heart failure), genetics and aging.4 These conditions are interlinked, reinforcing the concept that “AF begets AF”.4 In other words, the conditions that cause AF can worsen AF, and AF can also worsen these conditions. The main sequela to this is increased stroke risk. This is caused due to the irregular contractions of the left atria leading to stasis of blood, predisposing to thrombus formation. If the thrombus embolises, it can shift into the ventricle and enter systemic circulation and subsequently the carotid arteries, leading to the embolus becoming lodged in the cerebral arteries.
Beyond the arrhythmia, AF often signals broader pathological processes that impair cardiac function and reduce quality of life and life expectancy.5 Many of these conditions are closely linked to social determinants of health, disproportionately affecting populations with socioeconomic disadvantage. Effective AF management requires addressing both the arrhythmia and its underlying contributors.4
Symptoms
Like many cardiac conditions, AF symptoms can vary between individuals and overlap with other conditions, including coronary syndromes, heart failure, COPD and asthma. Common symptoms include5:
In addition, some individuals with AF may be completely asymptomatic.4
AF is also linked to higher rates of dementia and depression compared to the general population.5 Several tools are available to assess symptom burden and stratify the impact of symptoms, such as the modified European Heart Rhythm Association Score.5 Understanding the burden of AF and its associated comorbidities is essential for providing a holistic approach to patient care.
Stroke risk
The first sign of AF can be a stroke. The Australian Institute of Health and Welfare reported that in 2017–18, AF was present in 15.5% of patients hospitalised for stroke.1
Stroke risk varies, and the CHA2DS2-VA calculator is widely used in clinical practice to estimate the risk of stroke in AF.6 Points are assigned based on the following parameters7:
Scores range from 0 (ischaemic stroke incidence rate of 0.5 per 100 patient years) through to 8 (19.5 per 100 patient years).7 Scores may be used to inform decisions around initiating anticoagulation. There are other tools available, such as the GARFIELD-AF calculator, which offer more precise risk prediction, including bleeding and mortality, but require more detailed data.4
AF is diagnosed with the use of a 12-lead electrocardiogram (ECG). The ECG typically demonstrates an absence of discernible P waves and an irregularly irregular rhythm.5
Most recent international guidelines recommend further investigation for episodes lasting 30 seconds or more, with many anticoagulant trials requiring at least two separate ECGs demonstrating AF.5 Ambulatory monitors (e.g. Holter monitor) can be used for periods of 24 hours to a week and should not be confused with personal wearable devices.5
It is considered good practice to opportunistically screen for AF in patients ≥65 years of age or Aboriginal and Torres Strait Islander patients ≥50 years of age.8,9 Pharmacists may have the opportunity to do so when performing a blood pressure check, however it should be noted that automatic blood pressure machines may not always reliably detect the presence of AF.9
Wearable devices
TGA-approved wearable smart watches and devices are appropriate tools to assist in screening for AF,10 although diagnosis needs to be confirmed by an ECG that has been interpreted by a physician.5
Atrial flutter versus atrial fibrillation
Atrial flutter, a separate diagnosis to AF, is characterised as an atrial tachyarrhythmia but with regular atrial and ventricular activity. Nearly half of those diagnosed with atrial flutter will progress to atrial fibrillation.5 While stroke risk is elevated, it is not always elevated to the extent of AF.5
To address underlying causes or factors contributing to AF, tests recommended at diagnosis include5:
Further tests (e.g. for obstructive sleep apnoea and coronary artery disease) may be required for some patients to optimise management and improve outcomes.5
Treatments
The latest European Society of Cardiology (ESC) guidelines introduced the AF-CARE pathway, which emphasises treating contributing comorbidities and adopting a holistic person-centred approach to AF management.5 This replaces the previous ABC approach (Anticoagulation, Better symptom control, and Comorbidity management).5
C – Comorbidity and risk factor management
As outlined, many comorbidities increase the risk of developing AF, and contribute to increased risk of stroke (e.g. diabetes, hypertension, heart failure). Monitoring and managing these conditions is a priority in AF. Class 1 recommendations include5:
A – Avoid stroke and thromboembolism
Stroke risk assessment is important for determining anticoagulation needs. Across all guidelines there is consensus supporting anticoagulation for CHA2DS2-VA ≥2.4,5,11,12 There is less evidence for anticoagulant use in lower risk scores. In all cases, ongoing risk assessment and shared decision-making in balancing modifiable and non-modifiable risks for stroke and bleeding are key for successful management.5
R – Reduce symptoms by rate and rhythm control
Many patients with AF require interventions or treatments that control heart rate, revert to sinus rhythm or maintain sinus rhythm, leading to improved symptoms and outcomes.5 Treatment options include5:
E – Evaluation and dynamic reassessment
The ‘newest’ addition to previous treatment pathways ensures management adapts to changes in stroke risk, symptoms, comorbidities and other individual needs.5 Generally, a 6–12 monthly follow-up is recommended.5 Further guidance is available from the Quality Use of Medicines Alliance clinical guidance at https://go.medcast.com.au/anticoagulant-management-atrial-fibrillation-clinical-guide.
The role of anticoagulant therapy
AF significantly increases the risk of stroke, making timely assessment and anticoagulation critical. Oral anticoagulants reduce the risk of stroke by 64% and all-cause mortality by 26% in patients with AF.13,14
Direct-acting oral anticoagulants (DOACs)
DOACs have transformed ischaemic stroke prevention in AF (excluding patients with moderate/severe mitral stenosis or mechanical heart valves).5
Landmark trials (RE-LY, Rocket AF, and Aristotle) demonstrated their non-inferiority to warfarin in reducing the risk of stroke and systemic embolism, while halving the risk of intracranial haemorrhage.5
While DOACs offer advantages, no direct comparisons exist between apixaban, rivaroxaban and dabigatran. Choice of agent relies heavily on patient-specific factors such as age, renal function, comorbidities and bleeding risk, as well as practical considerations like accessibility and practicality of dosing regimens.
While stroke prevention benefits are well-established, prescribers must also address potential harms, including bleeding risk. Guidelines recommend addressing bleeding risk factors such as: discontinuing NSAIDs, reducing alcohol intake, lowering falls risk, and ceasing concomitant antiplatelets >12 months post-MI.4,5
However, limitations in the current DOAC evidence base warrant careful consideration. For instance, challenges remain for patients with extremes of bodyweight (BMI) above 40 kg/m² or >120 kg, where data on safety and efficacy remain sparse.4 Additionally, DOACs’ short half-lives mean anticoagulation will be compromised with any missed doses or therapy interruptions.15 Table 1 provides information on currently available oral anticoagulants.16
Warfarin
While DOACs are recommended over vitamin K antagonists (VKA) to prevent ischaemic stroke and thromboembolism in AF, patients with mechanical heart valves or moderate-to-severe mitral stenosis and AF should be anticoagulated with a VKA such as warfarin.5 Pharmacists may support patients prescribed warfarin by taking time to discuss their INR target range, the importance of consistent INR recording, and by providing strategies to improve INR control.
Role of the electrophysiologists
Electrophysiologists are cardiologists specialising in arrhythmias and rhythm control procedures such as catheter ablations. They practise in both public and private settings, and are often consulted for difficult-to-treat AF. While cardiologist referral is important for follow-up and treatment escalation, it should not delay assessing risk and commencing anticoagulation or arrhythmia treatments.
Role of the GP
GPs are integral to diagnosis and commencing the initial management of AF, as well as commencing appropriate therapies and specialist referral. Importantly, comorbidity diagnosis and ongoing management are also central to the GP role.
Role of the pharmacist
Stroke and bleeding risk change over time and may be influenced by new medical conditions or medicines that increase or decrease anticoagulant activity. Pharmacists play a pivotal role in addressing these issues by providing advice on day-to-day medicine use, reducing risks such as bleeding, medicine interactions and ongoing monitoring. Like all chronic conditions, adherence to risk-reducing therapies is an ongoing challenge, and there are a range of mitigating strategies pharmacists can use.17 Pharmacists may consider offering tailored solutions to suit individual needs – this might be in the form of dose administration aids or dose reminders. Encouraging Home Medicines Reviews and supporting patients to keep an up-to-date medicines list can all encourage patients’ self-advocacy and clinicians’ decision-making. Tools like the PSA’s Quick Reference Guide can further aid pharmacists in optimising medicine use. See www.psa.org.au/career-and-support/qum/qum-alliance/oral-anticoagulants/
All patients with recent presentations for AF may be eligible for publicly funded cardiac rehabilitation, which combines education, exercise assessments and ongoing planning by a multidisciplinary team. These programs improve exercise tolerance, support weight loss and promote physical activity – all key AF management strategies.5 Many centres also offer ongoing exercise therapy or referral to tailored programs. All health professionals can refer patients, and the Heart Foundation provides an Australia-wide cardiac rehabilitation directory. Further information on these centres is available at: www.heartfoundation.org.au/your-heart/cardiac-services-directory.
Pharmacists have an essential role in providing medicines education to individuals who are prescribed anticoagulant medicines. Education should be patient-centred, culturally appropriate and include details on the importance of adherence, expected side effects and potential drug interactions. Pharmacists can offer personalised education on minimising bleeding risk by recommending reduced alcohol consumption, avoiding NSAIDs and addressing fall prevention strategies. Incorporating broader cardiovascular risk advice, like smoking cessation, weight management, and promoting blood pressure and diabetes control, may improve AF outcomes. Patients with AF can be offered further support in the form of an anticoagulation plan. A sample anticoagulation plan is available at https://go.medcast.com.au/anticoagulant-care-plan. It is essential that anticoagulants are dosed in accordance with patient characteristics. Pharmacists should flag patients who may benefit from dose adjustment based on weight, renal function or age. When appropriate, patients can be referred to their local cardiac rehabilitation centres.
Given the increasing prevalence of AF, the importance of individualised anticoagulant treatment plans cannot be overstated. Pharmacists can support early detection of AF in at-risk patients and optimise use of oral anticoagulants through medication management services, patient education and ongoing monitoring. By working collaboratively as part of the multidisciplinary team, pharmacists can significantly impact the care of patients with AF.
| Case scenario continued Prior to dispensing Mrs Alvarez her apixaban, you assess the prescribed dose. You ask her if she would mind being weighed and record her weight as 57 kg. Given her age (≥80 years) and low weight (<60 kg), you identify that she meets the criteria for a dose reduction of apixaban to 2.5 mg twice daily, regardless of her renal function. You contact the prescriber, who agrees to the dose reduction. During the conversation, you also raise your concern about the elevated bleeding risk with the concurrent use of aspirin. The prescriber confirms the intention was to discontinue aspirin before starting apixaban. You then counsel Mrs Alvarez on her updated medication regimen. You discuss the importance of adherence, signs of bleeding and stroke, and strategies for fall prevention to ensure safe and effective anticoagulation therapy. |
Adam Livori BAppSci(NucMed), BPharm(Hons), MClinPharm, FSCANZ, FAdPha, FANZCAP(Cardiol, Research) is a cardiology pharmacist and the Lead Pharmacist for Medicine and Continuing Care at Grampians Health.
Jarrah Anderson BPharm is a Clinical Lead at Medcast.
Rawa Osman MPharm, MClinTria(Res), FSHPA, FANZCAP (MedsMgmt, PublicHlth) is a Director at QUM Connect, and Research and Design Lead for the Quality Use of Medicines Alliance.
Julie Briggs MPS (she/her) B Pharm, CredPharm (MMR), FANZCAP (Generalist, PublicHlth)
Rawa Osman is currently Design Lead for the Quality Use of Medicines Alliance, which is leading a national program focused on oral anticoagulants used in AF.
[post_title] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [post_excerpt] => Atrial fibrillation is the most common recurrent arrhythmia worldwide, and can put patients at increased risk of stroke. [post_status] => publish [comment_status] => open [ping_status] => open [post_password] => [post_name] => balancing-the-scale-the-role-of-oral-anticoagulants-in-atrial-fibrillation [to_ping] => [pinged] => [post_modified] => 2025-06-25 16:14:57 [post_modified_gmt] => 2025-06-25 06:14:57 [post_content_filtered] => [post_parent] => 0 [guid] => https://www.australianpharmacist.com.au/?p=29266 [menu_order] => 0 [post_type] => post [post_mime_type] => [comment_count] => 0 [filter] => raw ) [title_attribute] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [title] => Balancing the scale: the role of oral anticoagulants in atrial fibrillation [href] => https://www.australianpharmacist.com.au/balancing-the-scale-the-role-of-oral-anticoagulants-in-atrial-fibrillation/ [module_atts:td_module:private] => Array ( ) [td_review:protected] => Array ( [td_post_template] => single_template_4 ) [is_review:protected] => [post_thumb_id:protected] => 29742 [authorType] => )Get your weekly dose of the news and research you need to help advance your practice.
Protected by Google reCAPTCHA v3.
Australian Pharmacist is the official journal for Pharmaceutical Society of Australia Ltd.




