









Case scenario
Maggie, 34 years old, comes into the pharmacy requesting treatment for migraine, previously diagnosed by a doctor.
She typically experiences, 1–2 attacks per month and wants something simple and fast-acting to help relieve the pain when it presents. She has previously taken paracetamol but found that it didn’t help on its own.
Learning objectivesAfter reading this article, pharmacists should be able to:
Competency standards (2016) addressed: 1.1, 1.3, 1.4, 1.5, 2.2, 2.3, 3.1, 3.2, 3.3, 3.5 Accreditation number: PSAAP2606CP Accreditation expiry: 30/06/2028 |
Already read the CPD in the journal? Scroll to the bottom to SUBMIT ANSWERS.
Introduction
If you feel like you talk about headaches all day, you’re probably right. Headache is a common reason for patients to present to pharmacy.1 But without guidance, they may cycle through the same options, even if they’re not providing the relief they need. It’s one reason the burden of headache remains substantial – including impaired quality of life, decreased productivity, financial costs, and psychosocial impacts on employment, relationships and mental health.2 Recent global data has also highlighted the high level of under-reporting, under-diagnosis and under-management of migraine, meaning that many opportunities for early and effective intervention are missed.3
As accessible community healthcare providers, pharmacists are well placed to support recommendations for the selection and optimal use of medicines, provide advice, and assist patients to improve prophylaxis adherence.1,4,5 This should be in the context of a wider management plan involving control of known modifiable triggers, and correction of suboptimal cycles of treatment that can lead to medication overuse headache (MOH), particularly with migraine.4,6
Common primary headache phenotypes and the inflammatory thread
Headaches are broadly divided into primary and secondary types.5,7 Primary disorders, mainly migraine and tension-type headache (TTH), less often cluster headaches, account for nearly 98% of cases and are the most common headache presentations seen in primary care.5,7 Differentiating features of these headaches are listed in Table 1.
The inflammatory thread
Inflammation plays a crucial role in the pathophysiology of both TTH and migraine, and is recognised as a shared mechanism across the most common primary headache types although the mechanisms differ.9,10 TTH is more heavily associated with the activation and sensitisation of peripheral nociceptors in myofascial tissues around the head and neck, while migraine involves a pronounced, acute neurogenic inflammation in the meningeal vasculature.9,10
These mechanisms provide a pharmacological rationale for cyclooxygenase inhibition to reduce prostaglandin-mediated pain transmission at peripheral and central sites.9,11 Non-steroidal anti-inflammatory drugs (NSAIDs) address these inflammatory components while also exerting antipyretic and analgesic effects.9,11 This aligns with guideline recommendations that place NSAIDs among first-line options for infrequent acute TTH and migraine if there are no contraindications.12,13
Table 1 – Differentiating features of common primary headache types
 4 steps to optimising headache management
4 steps to optimising headache management
Recognising that neuroinflammatory processes contribute to common primary headaches, here is a 4-step practical guide for managing these presentations in pharmacy.
1. Conduct a structured assessment: history, examination and red flags
Even in a busy pharmacy environment, assessing the patient can be as simple as asking about the headache and relevant history, and you may be the first healthcare professional that’s taken the time to ask. A structured history-taking for all patients presenting or enquiring about headache related symptoms helps with screening, assessing ‘red flags’ and recommending appropriate treatment or referrals.
Information that should be captured during history-taking includes8:
- severity
- duration
- onset (e.g. sudden or slowly worsening)
- location (e.g. one or both sides of the head, whether it always affects the same side if unilateral)
- character (e.g. pulsating, stabbing, throbbing, squeezing, tightness, pressure)
- frequency and pattern of occurrence (e.g. same time each day or month)
- impact on daily activities (e.g. work, social life, family, exercise, sleep)
- aggravating and mitigating factors (e.g. exacerbated by movement or positional changes, relieved by resting in a dark room)
- precipitating factors (e.g. head or neck trauma)
- triggers (e.g. exertion, alcohol, menstruation, diet, stress)
- associated symptoms (e.g. nausea, vomiting, neck tension/pain, sensitivity to light, sound or odours, presence of aura or focal neurological symptoms, other systemic features)
- medication history (ask about previously used acute or preventive drugs for headache – specifically drug, dose, response and frequency of use)
- personal and family history of headaches (e.g. migraine and cluster headaches can be familial)
- relevant comorbidities (e.g. pregnancy or postpartum, cancer, human immunodeficiency virus (HIV)).
Some cases may require urgent referral to a medical practitioner for further assessment and/or investigation, including physical examination, to exclude serious secondary causes of headache. Red flag features suggestive of a secondary or potentially serious cause of headache can be systematically screened using tools such
as SNNOOP10.7,14
‘Red flag’ assessment with SNNOOP107,14
The SNNOOP10 mnemonic is a structured checklist used in headache assessment to help clinicians rapidly identify red flags that may indicate a secondary or potentially serious cause of headache.
S – Systemic symptoms (fever, weight loss)
N – Neoplasm history
N – Neurologic deficit or dysfunction
O – Onset sudden/abrupt (thunderclap headache)
O – Older age at onset (typically >50 years)
P – Pattern change or recent onset of headache
P – Positional headache
P – Precipitated by sneezing, coughing or exercise
P – Papilloedema
P – Progressive or atypical presentation
P – Pregnancy or postpartum
P – Painful eye with autonomic features
P – Posttraumatic onset of headache
P – Pathology of the immune system (e.g. human immunodeficiency virus (HIV])
P – Painkiller overuse or new medicine recently initiated
In addition to SNNOOP10, other reasons for referral can include8:
- migraine symptoms increasing in frequency or occurring ≥3 days
a month - recent onset of headache in a person with cancer or a history of cancer
- recent onset of headache in a child
<5 years old - symptoms of dehydration and/or electrolyte disturbance as a result
of vomiting - headaches not responding to appropriate treatment.
- Refer to the APF Headache and migraine treatment guideline8 for further information.
In the absence of red flags and with a phenotype consistent with a primary headache disorder, imaging is usually unnecessary.7,15
2. Define management goals with the patient, including prevention of MOH
Acknowledging the wide-ranging impacts of the patient’s headaches is important for developing a collaborative approach to headache management and encouraging treatment adherence.6 For most patients, management goals for primary headaches will include4,6,12,13:
- Acute treatment – rapid and sustained relief of acute symptoms
- This includes prevention/treatment of medication overuse headache
- Trigger identification/avoidance and lifestyle measures – addressing predisposing, precipitating and/or perpetuating factors, typically identified through a headache diary
- Prophylaxis – reducing the severity/number of headaches and preventing chronicity in patients with frequent or debilitating attacks (this will require referral to their general practitioner for treatment).
More on medication overuse headache
MOH, also known as ‘analgesic rebound headache’, is a key, preventable driver of chronic headache and disability.16 Classified as a secondary headache, it occurs most commonly when patients with established primary headache disorders (mainly migraine or TTH) overuse acute treatments and inadvertently increase the frequency and intensity of their headaches, likely via central sensitisation.16
The latest medication limits recommended by the Therapeutic Guidelines for the prevention of MOH are ≤3 days per week and <10 days per month for simple non-opioid analgesics, and ≤2 days per week and <10 days per month for triptans.17
Where MOH is suspected (pre-existing headache disorder, headache ≥15 days per month, overuse of acute medications >3 months), patients may require initiation of appropriate prophylaxis alongside controlled medication withdrawal (e.g. via graded reduction in dose and frequency, or use of bridging therapy), plus psychological referral to address any psychological factors that may contribute to overuse behaviours.16,17
3. Reinforce lifestyle changes and non-pharmacological interventions as foundation therapy
Regular lifestyle habits play a key role in reducing migraine and TTH frequency. Helpful strategies include12,13:
- consistent sleep routines and good sleep hygiene
- regular meals and good nutrition to maintain stable blood glucose
- adequate hydration (1.5 to 2L of water daily) and limiting caffeine to <200 mg per day (approximately 2 cups of coffee)
- regular physical activity, aiming for 30–40 minutes of aerobic or resistance exercise 3–4 times a week
- optimising workplace ergonomics and taking short breaks to stretch and rest the eyes
- relaxation practices (e.g. meditation, mindfulness, breathing exercises, yoga)
- avoiding or managing known triggers, including dietary triggers or sensory sensitivities (e.g. earplugs for noise sensitivity, tinted lenses for light sensitivity).
Acute non-pharmacological measures should also be recommended to all patients, including cold packs over the forehead or back of skull, hot packs over the neck and shoulders, neck stretches/self-mobilisation, and resting in a quiet dark room.12,13 Referral for physiotherapy, acupuncture, or psychotherapy may also be indicated in some patients.12,13
4. Support appropriate use of acute pharmacotherapy, with a stepwise approach to optimise self‑management
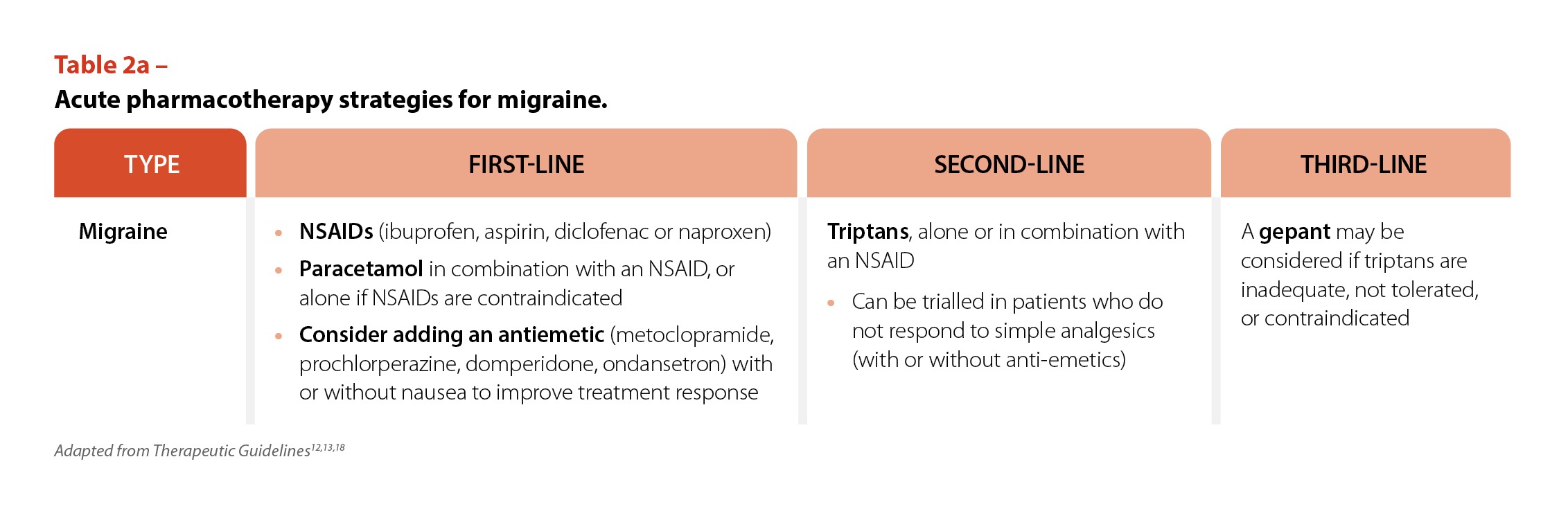
Therapeutic Guidelines for migraine supports the use of non-opioid analgesics (i.e. an oral NSAID with or without paracetamol), as first-line acute treatment.12,13 Table 2a and 2b provide guideline-recommended, stepwise pharmacotherapy strategies for both headache types.12,13,18 Opioid analgesics are not recommended for either condition and should be avoided.12,13
 Evaluating relative risk profiles when selecting an NSAID
Evaluating relative risk profiles when selecting an NSAID
The benefit-risk balance of individual NSAIDs is mainly driven by their gastrointestinal (GI) and cardiovascular safety profile. To determine if NSAIDs are appropriate for acute headache pain, pharmacists should consider individual patient risk factors, potential drug interactions, alongside the renal, cardiovascular and GI risk profiles of each NSAID option.19,20
All NSAIDs can cause serious GI adverse effects (e.g. peptic ulcer perforations, obstructions and bleeding) and are associated with an increased risk of cardiovascular events and impaired renal function, particularly at prescription doses. GI risk may be particularly top of mind for both patients and clinicians, given some of the most reported adverse events are GI in nature.20 Selective NSAIDs generally have a lower risk of GI complications compared with non-selective NSAIDs. Among non-selective NSAIDs, piroxicam appears to carry the greatest GI risk, whereas ibuprofen and diclofenac are associated with comparatively lower risks. However, this advantage is lost for ibuprofen when used at higher doses, above over-the-counter pack instructions. In a meta-analysis evaluating GI risks associated with non-selective NSAIDs according to dose, ibuprofen at standard over-the-counter doses (<1200mg/day, e.g. 400mg three times a day) was found to have the lowest risk of developing upper GI bleeding compared to diclofenac, naproxen, indomethacin and piroxicam.21,22 Other data support ibuprofen, taken at short-term standard over-the-counter doses in otherwise healthy patients without precautions or contraindications, as having an overall GI tolerability similar to paracetamol.23-25 These findings contrast with the higher GI risk associated with prolonged, high‑dose NSAID use, and with the additional risk commonly seen in older or patients with comorbidities.18,26
Consider NSAIDs early in the treatment pathway
Non-prescription NSAIDs (e.g. ibuprofen, diclofenac, naproxen) are considered a suitable first-line self-management strategy for appropriate patients requiring analgesia for primary headache.12,13 In a 2024 network meta-analysis evaluating the efficacy and safety of simple analgesics for episodic TTH, data from six randomised, controlled clinical trials (n=3,507) found that ibuprofen 400 mg had the highest probability of pain relief at 2 hours (91.7%) followed by diclofenac-K 12.5 and 25 mg (83.3%).27 For the treatment of acute migraine, a 2024 systematic review and meta-analysis of NSAIDs and triptans using sumatriptan as a reference found that, out of the NSAIDs studied (ibuprofen, diclofenac-K, naproxen sodium and celecoxib), ibuprofen had a high likelihood of pain freedom from 2–24 hours.28
In recommending ibuprofen to patients, explain that taking with food can delay absorption and is likely to delay early onset of ibuprofen, which is particularly relevant for patients who value rapid relief.29 Furthermore, there are instances where other NSAID selections may be more appropriate. For instance, the Therapeutic Guidelines suggest naproxen may be more effective for hormone-related migraine such as menstrual migraine.13 Overall choice of drug for acute treatment depends on efficacy, tolerability, severity
of the attack, other presenting symptoms and comorbidities.
The formulation of an NSAID can also impact absorption. Pharmacokinetic data show that salt forms (e.g. ibuprofen sodium) and liquid capsule formulations reach therapeutic plasma levels more quickly than standard ibuprofen acid.30 For migraine, where early intervention is crucial, advising patients to take a fast-absorbing ibuprofen formulation at the first sign of pain – ideally on an empty stomach for standard over-the-counter doses, if tolerated – may be appropriate.20,29 However, administration with food may be more appropriate for individuals who experience GI discomfort when taking NSAIDs on an empty stomach.20
Combination non-opioid analgesics with synergistic potential, such as ibuprofen with paracetamol, may be under-utilised in acute headache management. Fixed-dose combinations of ibuprofen and paracetamol offer an alternative treatment option that combines the anti-inflammatory and peripheral analgesic effects of ibuprofen with central actions of paracetamol.31,32 Establishing a place for fixed-dose ibuprofen and paracetamol, either as first-line analgesia, or as the first step up from monotherapy (rather than progressing directly to prescription analgesics)– can align real-world practice with evidence and provide patients with more options to optimise self-management, particularly
if they find monotherapy insufficient.13
Regardless of the analgesic chosen, clear instructions on optimal dosing is critical. For acute migraine, early treatment at the onset of pain is much more likely to be effective.13 For both migraine and TTH, advise patients about excessive medication use and to limit use of analgesics to <10 days per month to avoid the risk of MOH.16,17
Knowledge to practice
Before recommending treatment, it is beneficial to take a structured history and to rule out red flags necessitating referral to a doctor. Understanding the nature and impact of headache and patient preferences for treatment helps guide suitable treatment recommendations.
As experts in medicines, pharmacists are well placed to educate patients on appropriate management and steps to avoid MOH. As patients may not be aware of the treatment ladder, advising on which medicines, formulations and combinations to trial before escalating to second-line options remains a key role of pharmacists.
Conclusion
Helping patients to navigate therapies and utilise them appropriately is a key role for pharmacists. By knowing and explaining the underlying mechanisms of headache and migraine, treatment options and how to move through and combine them, pharmacists can help reduce their impact in the community.
Case scenario continued
Following history-taking and screening with SNNOOP10, no contraindications to NSAIDs or red flags are identified. Her symptoms are consistent with migraine without aura. For acute treatment of her next attack, you recommend a fast-absorbing NSAID formulation. For example, ibuprofen sodium or a liquid capsule with a glass of water, ideally taken on an empty stomach, if tolerated, to optimise absorption. You encourage taking the medicine as soon as the pain presents. You also encourage non-pharmacological strategies, such as resting in a quiet, dark environment at the onset of migraine symptoms. You discuss medication overuse headache thresholds and trigger management through lifestyle changes. You advise Maggie to come back to the pharmacy if she needs further step-up to her treatment or if headache frequency, severity or associated disability increases.
Key points
- Pharmacists are a primary touchpoint for patients presenting with headache and migraine.
- Inflammation is a shared inflammatory thread in TTH and migraine, therefore NSAIDs are among first-line options for infrequent acute TTH and migraine if there are no contraindications.
- For patients who need step-up treatment, combination therapy with an NSAID and paracetamol provides another option for treatment.
Our Author
Dr Catherine Panwar (she/her) PhD (Science), BSc (Biotech), Hons. has nearly 20 years’ experience in medical communications and is the founder and Director of Panwar Health, a medical communications company.
Conflict of interest
Cat Panwar is a paid consultant for Reckitt Benckiser.
None to declare for reviewer.
Our reviewer
Amanda Quek (she/her) PhD, BPharm (Hons I), GradCertAppPharmPrac, GradCertDMed
References
- BaniHani H, Lampl C, MaassenvandenBrink A, et al. The role of community pharmacists in managing common headache disorders, and their integration within structured headache services: position statement on behalf of the European Headache Federation (EHF) and Lifting The Burden (LTB: the Global Campaign against Headache), with the formal endorsement of the International Pharmaceutical Federation. J Headache Pain 2025;26(1):100.
- World Health Organization. Migraine and other headache disorders. 2025. At: who.int/news-room/fact-sheets/detail/headache-disorders
- Lanteri-Minet M, Leroux E, Katsarava Z, et al. Characterizing barriers to care in migraine: multicountry results from the Chronic Migraine Epidemiology and Outcomes – International (CaMEO-I) study. J Headache Pain 2024;25(1):134.
- Lee VME, Ang LL, Soon DTL, et al. The adult patient with headache. Singapore Med J 2018;59(8):399–406.
- Ahmed F. Headache disorders: differentiating and managing the common subtypes. Br J Pain 2012;6(3):124–32.
- Kitson J. Identifying and managing migraine in general practice. Prescriber 2021;32(5):15-20.
- Viera AJ, Antono B. Acute headache in adults: a diagnostic approach. Am Fam Physician 2022;106(3):260–68.
- Samson LN, ed. Headache and migraine. Australian Pharmaceutical formulary and handbook; [updated 28 Nov 2024]. At: https://apf.psa.org.au/treatment-guidelines-pharmacists/headache-and-migraine
- Bendtsen L, Ashina S, Moore A, et al. Muscles and their role in episodic tension-type headache: implications for treatment. Eur J Pain 2016;20(2):166–75.
- Morgan CT, Nkadimeng SM. The Role of Inflammation in Migraine Headaches: A Review. FASEB Bioadv. 2025;7(7):e70033.
- Pardutz A, Schoenen J. NSAIDs in the Acute Treatment of Migraine: A Review of Clinical and Experimental Data. Pharmaceuticals (Basel) 2010;3(6):1966–87.
- Tension-type headache. Therapeutic Guidelines; [published Dec 2025]. At: https://tgldcdp.tg.org.au/viewTopic?etgAccess=true&guidelinePage=Neurology&topicfile=tension-type-headache
- Therapeutic guidelines; [published Dec 2025].At: https://tgldcdp.tg.org.au/viewTopic?etgAccess=true&guidelinePage=Neurology&topicfile=acute-management-of-seizures-and-status-epilepticus&guidelinename=auto§ionId=c_NRG_Migraine_topic_17#c_NRG_Migraine_topic_17
- Do TP, Remmers A, Winther Schytz H, et al. Red and orange flags for secondary headaches in clinical practice: SNNOOP10 list. Neurology 2019;92(3):134–44.
- Headache classification and diagnosis. Therapeutic guidelines; [published Dec 2025]. At: https://tgldcdp.tg.org.au/viewTopic?etgAccess=true&guidelinePage=Neurology&topicfile=acute-management-of-seizures-and-status-epilepticus&guidelinename=auto§ionId=c_NRG_Headache-classification-and-diagnosis_topic_2#c_NRG_Headache-classification-and-diagnosis_topic_2
- Fischer MA, Jan A. Medication-Overuse Headache. StatPearls; [updated 2 Aug 2023]. At: ncbi.nlm.nih.gov/books/NBK538150/
- Medication overuse headache. Therapeutic guidelines; [published Dec 2025]. At: https://tgldcdp.tg.org.au/viewTopic?etgAccess=true&guidelinePage=Neurology&topicfile=medication-overuse-headache
- Nonopioid analgesics in pain management. Therapeutic guidelines; [updated Aug 2022). At: https://tgldcdp.tg.org.au/viewTopic?etgAccess=true&guidelinePage=Pain%20and%20Analgesia&topicfile=understanding-pain&guidelinename=auto§ionId=c_agg7-c38-s2-2#c_agg7-c38-s2-2
- Hopkins S, Yang V, Liew D, et al. Choosing a nonsteroidal anti-inflammatory drug for pain. Aust Prescr 2025;48(4):139–44.
- Buckley N, ed. Australian Medicines Handbook. 2026. At: https://amhonline.amh.net.au/
- Moore N, Pollack C, Butkerait P. Adverse drug reactions and drug-drug interactions with over-the-counter NSAIDs. Ther Clin Risk Manag 2015;11:1061–75.
- Lewis SC, Langman MJS, Laporte J, et al. Dose-response relationships between individual non-aspirin nonsteroidal anti-inflammatory drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on individual patient data. Br J Clin Pharmacol 2002;54(3):320–6.
- Moore N, Van Ganse E, Le-Parc J, et al. The PAIN Study: Paracetamol, Aspirin and Ibuprofen New Tolerability Study. Clin Drug Invest 1999;18(2):89–98.
- Varrassi G, Pergolizzi JV, Dowling P, et al. Ibuprofen Safety at the Golden Anniversary: Are all NSAIDs the Same? A Narrative Review. Adv Ther 2020;37(1):61–82.
- Rampal P, Moore N, Van Ganse EV, et al. Gastrointestinal tolerability of ibuprofen compared with paracetamol and aspirin at over-the-counter doses. J Int Med Res 2002;30(3):301–8.
- Marcum ZA, Hanlon JT. Recognizing the Risks of Chronic Nonsteroidal Anti-Inflammatory Drug Use in Older Adults. Ann Longterm Care 2010;18(9):24–7.
- Xie R, et al. Efficacy and safety of simple analgesics for acute treatment of episodic tension-type headache in adults: a network meta-analysis. Ann Med 2024;56(1):2357235.
- Karlsson W, Ostinelli EG, Zhuang ZA, et al. Comparative effects of drug interventions for the acute management of migraine episodes in adults: systematic review and network meta-analysis. BMJ 2024:386:e080107.
- Koenigsknecht MJ, Baker JR, Wen B, et al. In vivo dissolution and systemic absorption of immediate release ibuprofen in human gastrointestinal tract under fed and fasted conditions. Mol Pharm. 2017 Dec 4;14(12):4295-4304.
- Moore AR, Derry S, Straube S et al. Faster, higher, stronger? Evidence for formulation and efficacy for ibuprofen in acute pain. Pain 2014;155(1):14–21.
- Daniels SE, Goulder MA, Aspley S, et al. A randomised, five-parallel-group, placebo-controlled trial comparing the efficacy and tolerability of analgesic combinations including a novel single-tablet combination of ibuprofen/paracetamol for postoperative dental pain. Pain 2011;152(3):632–42.
- Mehlisch DR, Aspley S, Daniels SE, et al. A single-tablet fixed-dose combination of racemic ibuprofen/paracetamol in the management of moderate to severe postoperative dental pain in adult and adolescent patients: a multicenter, two-stage, randomized, double-blind, parallel-group, placebo-controlled, factorial study. Clin Ther 2010;32(6):1033–49.


