


 Ruth Nona[/caption]
Ruth Nona[/caption]

 Kate Gunthorpe MPS[/caption]
Kate Gunthorpe MPS[/caption]
 Madison Low[/caption]
Madison Low[/caption]


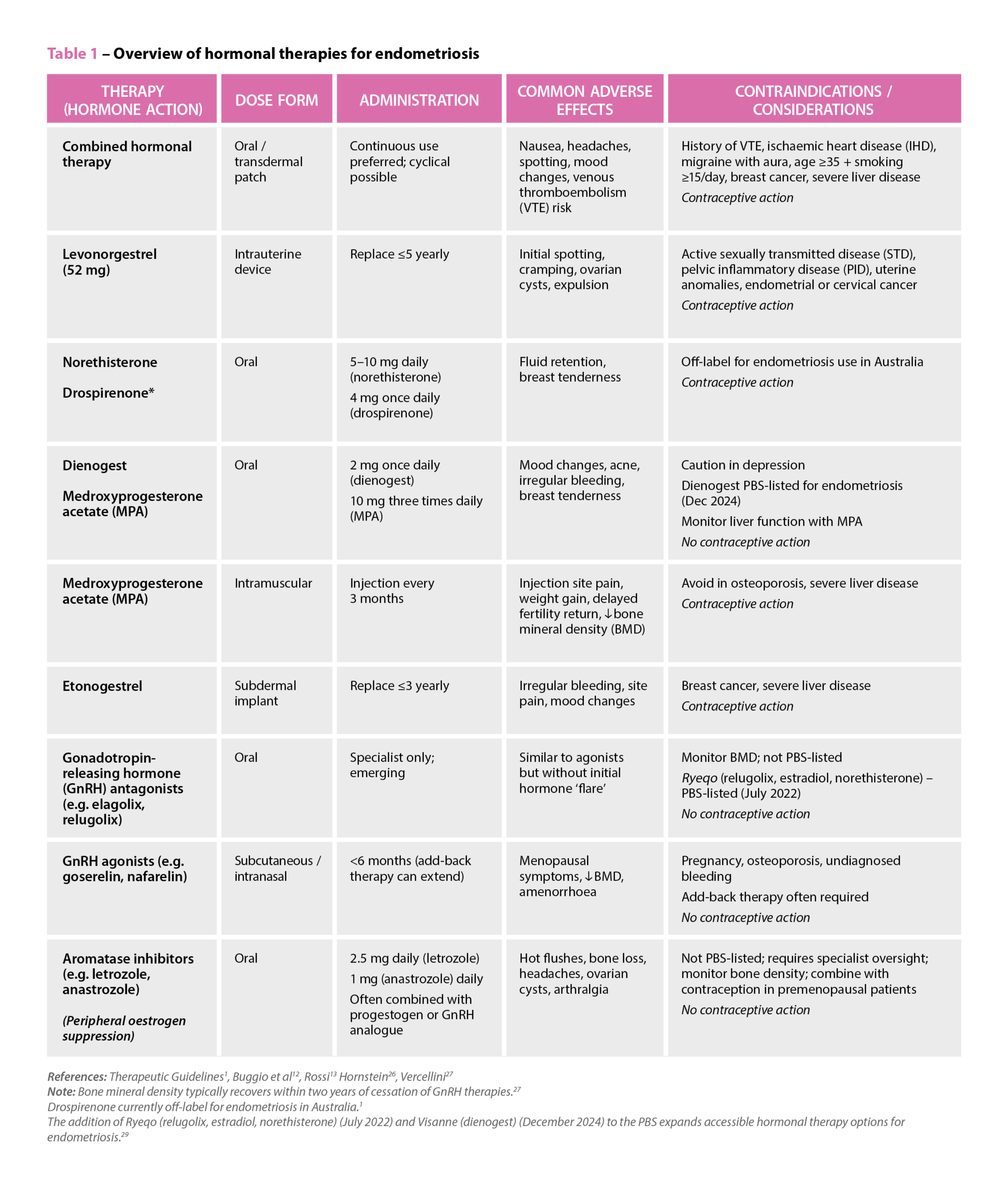 References: Therapeutic Guidelines
References: Therapeutic Guidelines
ADHD medicine poisonings have quadrupled in the last decade, new research has found.
In 2023, there were 3,242 reported poisoning cases involving ADHD medicines, more than four times the 795 cases recorded in 2014.
Drawing on national data from the NSW Poisons Information Centre (NSWPIC), researchers from the University of Sydney found that over half of the 17,000 self-reported cases during the study period led to hospitalisation, with more than 9,000 involving children under 15 years of age.
These numbers are also likely underreported, said lead researcher Amy Thomson.
‘While our study captured over 17,000 cases over 10 years, that only includes calls to the Poisons Information Centre – which means someone had to actually pick up the phone for advice,’ she said. ‘It doesn’t include cases where someone went straight to their doctor or called an ambulance without contacting the centre.’
Prescription trends linked to growing poisoning rates
There has been a significant uptick in ADHD diagnoses, with the number of Australians diagnosed with ADHD more than doubling between 2013–2020.
One of the main drivers behind the rise in ADHD medicine poisonings is the growing number of prescriptions being issued, Ms Thomson said.
‘The majority of agents we studied have shown increased poisoning incidents, but largely in proportion to the number of prescriptions being written,’ she said.
‘The exception is clonidine, where we’re seeing a much greater increase in poisonings compared with the number of prescriptions issued.’
Originally indicated for hypertension, clonidine has been found to be useful for some patients with ADHD when stimulants don’t adequately manage symptoms.
‘Around 35% of the poisoning cases were from clonidine, and another 35% were from methylphenidate (Ritalin), which is much more commonly prescribed,’ Ms Thomson said.
Unintentional overdoses most common in children
Unintentional poisoning from ADHD medicines are more likely to occur in children due to the high volume of prescribing in this age cohort, Ms Thomson said.
‘About 60% of [the reported] cases were unintentional – for example, where a parent doses a child, then the other parent, unaware, gives another dose. That kind of miscommunication can lead to hospitalisation, especially with clonidine,’ she said.
‘There are also cases of children being curious and getting into a sibling’s medication.’
Because clonidine is formulated for adults, dosing children often requires quarter or half tablets. ‘These are small white tablets that need to be cut manually, which increases the risk of dosing errors – for instance, giving a whole tablet instead of the intended half or quarter,’ she said.
Intentional poisonings, on the other hand, were more likely to occur among adolescents.
‘Concerningly, adolescent females are showing an increased risk of intentional poisoning with these medicines,’ Ms Thomson added.
Don’t call them lollies!
Awareness of ADHD has grown significantly, so it’s crucial for pharmacists to provide medicine safety counselling. This includes ensuring families know to store medicines safely and well out of reach of children, Ms Thomson advised.
‘Parents should be advised to avoid referring to medicines as “lollies” – if a parent convinces a child to take medicine by calling it a lolly, the child may later take more on their own,’ she said.
Pharmacists can also help parents establish clear communication strategies at home to avoid accidental double doses.
‘Life can be chaotic when you’re trying to get everyone ready for the school run, and it’s very easy for both parents to dose one child or to dose the incorrect child,’ Ms Thomson said.
Encouraging families to document each dose or use a shared communication system could help.
‘Pharmacists know their patients and are best placed to help them find a system that works,’ she said.
For clonidine use in children, there should ideally be a change at a national level, with the development of a suitable paediatric formulation, Ms Thomson thinks.
But in the interim, there are some ways pharmacists could help to prevent dosing errors.
‘At a pharmacy level, it may be appropriate in some cases for pharmacists to divide tablets ahead of time and supply them in dose administration aids, which could help some families,’ she said.
Pharmacists also play an important role in harm minimisation for adolescent patients, particularly when the adolescent is old enough to collect their own prescription – generally those aged 16 years and over in NSW.
‘The pharmacist can have a conversation about maturity, the level of supervision required, and what’s appropriate for that patient,’ Ms Thomson said.
Pharmacists have an important role in triage if double dosing or poisoning is suspected.
‘If the child is not breathing, has collapsed, or is unconscious, direct the parent to call 000 immediately,’ she said.
‘Otherwise, the pharmacist should refer them to call the Poisons Information Centre on 13 11 26, which is a 24/7 national hotline operating every day of the year. It’s staffed by pharmacists who specialise in poisoning management, who can triage and provide advice.’
Ms Thomson emphasised that there is no wrong referral. ‘If a parent calls and the child turns out to be fine, that’s a good outcome.’

