



")





Medication reviews have been improving the lives of patients and boosting the careers of pharmacists for a quarter of a century, with the future of the service looking even brighter.
In February 1997, Debbie Rigby FPS, Lesley Taylor MPS and Roger Kilpatrick were among the first Australian pharmacists to be accredited by the Australian Association of Consultant Pharmacy (AACP) to conduct medication reviews.
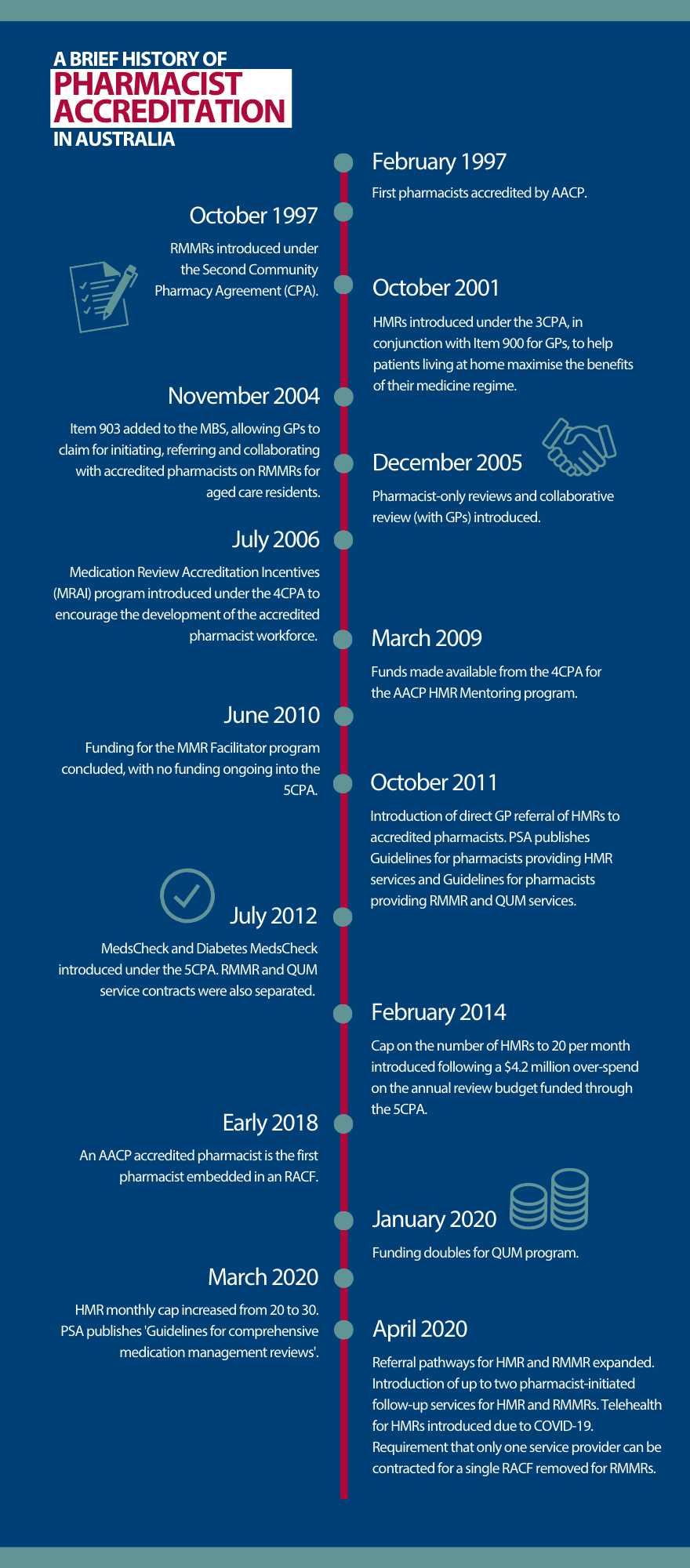
That year, federal government funding for Residential Medication Management Reviews (RMMRs) and medication reviews for war veterans began. Funding for Home Medicines Reviews (HMRs) began in 2001.
‘I went to a course in Melbourne before a conference, and we basically did the whole [accreditation] workshop in 2 days,’ said Ms Taylor, who is based in the New South Wales coastal town of Port Macquarie. ‘Then I came home, did a couple of [RMMRs] and handed those in for marking.’

Since 2007, the government has funded 1,112,338 HMRs. This includes more than 30,000 first and 8,600 second follow ups since April 2020.
During the same period, more than 1.66 million RMMRs have been conducted with Quality Use of Medicines (QUM) services in more than 2,950 residential aged care facilities (RACFs).
Accreditation has enabled innovative models of care, such as embedded pharmacists in aged care, Aboriginal Community Controlled Health Organisations and general practice, said PSA National President Associate Professor Chris Freeman.
‘I’m confident these roles would not exist without the work and reputation accredited pharmacists have earned over the past 25 years,’ he added.
Improving professional standards and medicine safety
Accreditation was set up as a ‘hurdle’ to ensure a certain standard of care, said Col. (Rtd) Bill Kelly AM FPS, who served as CEO of AACP from 2003–2009.
‘If there is going to be remuneration for a program or process, there has to be some control over the level of quality of the service provided and the people providing it,’ he said.

‘Pharmacists were not only required to update their clinical skills [through accreditation] but then every 3 years through reaccreditation. This maintains the quality of the reviews and that, of course, always leads to better outcomes.’
Medication reviews also introduced the notion of collaboration, Col. Kelly said.
‘That was the start of working together with other health providers to improve patient outcomes in the area of medicine management,’ he added.
Accredited pharmacists conducting medication reviews support QUM and improve medicine safety, said Sarah Gillespie MPS, AACP Clinical Service Manager. While conducting reviews, they empower and educate patients and their carers to better understand and manage their medicines.
‘Accredited pharmacists can identify medicine-related problems and potentially inappropriate medicines during a medication review,’ she said. ‘They also can identify medicines that may no longer be of benefit or may be causing harm, and can provide suggestions for deprescribing.’
How were medication reviews received?
Reflecting on the perception of RMMRs in the early days, Ms Taylor said there was some initial resistance from RACF staff and nurse unit managers.
Over time, however, these relationships improved.
‘I’m confident these roles would not exist without the work and reputation accredited pharmacists have earned over the past 25 years.’
A/Prof Chris Freeman
‘We made them aware that they had some input as well, because they saw the patient every day, so they had more of an idea than someone who sits in for an hour or two,’ she said.
‘They would have suggestions, for example, “Why would the GP add [this medicine]?” Or “This one isn’t working, is there something else we can do?”’
Ms Taylor described RMMRs as a ‘stepping stone’ to demonstrate the value pharmacists can add in medicine management.
‘GPs are more accepting of HMRs now,’ she said. ‘It took a while to gain their trust and [for them] to know that we weren’t looking over their shoulder, but trying to give the patient more opportunities to express the way they wanted their medicines managed.’
As one of the only accredited pharmacists who performs HMRs on a regular basis in Port Macquarie, she has a great rapport with local doctors.
‘There are a few who refer to me personally, and you tend to get more repeat business from them too,’ she said.
Despite their successes in Australia, however, RMMRs and HMRs remain ‘significantly underutilised’, Ms Rigby said.
Only 1 in 7 people aged 75 years or more with polypharmacy receives a medication review in a 12-month period, and only 4% of veterans who regularly use medicines receive an HMR. Alarmingly, Ms Rigby said only 1 in 5 residents in aged care receive an RMMR within 90 days of admission.
Remuneration for medication reviews
RMMRs and HMRs can be profitable for pharmacists and pharmacy owners, said pharmacy business consultant Bruce Annabel. It just depends on how they are approached.

Pharmacists who perform many RMMRs are paid well above the award, often upwards of $50 per hour. They receive 80% of the fee to perform an RMMR, as well as 80% of the QUM fee.
There are three core ways HMRs are approached, Mr Annabel said. The ‘benchmark’ is pharmacists who see them as central to their health offer and a communication tool to demonstrate the value they provide to patients and the community.
‘They do it because of the professional reward of helping people,’ Mr Annabel said. ‘But they also make money out of them, because they don’t see [HMRs] as being incidental to the standard pharmacy dispensing offer.’
As professional services such as HMRs are common practice for these pharmacies, their processes and systems are fine tuned and efficient, rendering them profitable and important to the overall attraction of the pharmacy.
The second level is when employed accredited pharmacists perform HMRs ‘here and there’. Most pharmacies fall into this category, Mr Annabel said.
While pharmacists who provide this service ad hoc see it as valuable to the community, it is not particularly lucrative.
‘As they don’t do many [HMRs], they tend not to do them particularly efficiently,’ Mr Annabel said. ‘They’re lucky to break even.’
The third level of HMR, when pharmacies receive ongoing referrals, involves outsourcing to a contractor.
‘This is an individual accredited pharmacist who runs their own business and [potentially] contracts for a number of pharmacies doing HMRs on their behalf,’ he said.
Pharmacies that provide this service receive a modest fee, but accredited pharmacists who perform this service can perform HMRs as efficiently and effectively as those in the first group.
There is, however, a negative aspect to this model.
‘Because it’s not being [performed] by someone who’s associated with that pharmacy, the owners get less of the knock-on promotional and recognition benefits,’ Mr Annabel said.
Becoming and remaining accredited to perform RMMRs and HMRs can be an arduous process. While it is a professional passion for many, Mr Annabel said that’s not enough.
‘I think it needs to be well remunerated, given the higher expertise, training [and] accreditation requirements, and the risk factor in [performing them] correctly,’ he said.
Looking forward
Removing barriers that stop more pharmacists gaining accreditation and supporting the growing number of older, at-risk Australians through these services remains a key area of focus for PSA.
‘As of January 2022, Australia has over 2,000 accredited pharmacists across the nation,’ said A/Prof Freeman. ‘However, given the high demand for this service and the clear gap between those who need a medication review and those [who] have received one, we need more pharmacists to become accredited.’
There are many opportunities for accredited pharmacists to conduct medication reviews, Ms Gillespie agreed.
‘Recent expansions to program rules allow for certain designated non-GPs, such as psychiatrists, pain specialists and palliative care physicians to refer, along with follow-up reviews, increased caps and telehealth consultations in 2020,’ she said.
The PSA is also striving to remove service caps, shift HMRs and RMMRs into the MBS and secure rebates for pharmacists to contribute to interdisciplinary case conferencing.
‘To help make this a reality – and ensure your voice is heard – I encourage all accredited pharmacists, current and prospective, to join the Interdisciplinary Team-Based Care Community of Specialty Interest,’ A/Prof Freeman added.
