
The social highlight of the annual PSA conference is the Gala Dinner, and this year certainly did not disappoint.


td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32437
[post_author] => 3410
[post_date] => 2026-06-24 11:53:45
[post_date_gmt] => 2026-06-24 01:53:45
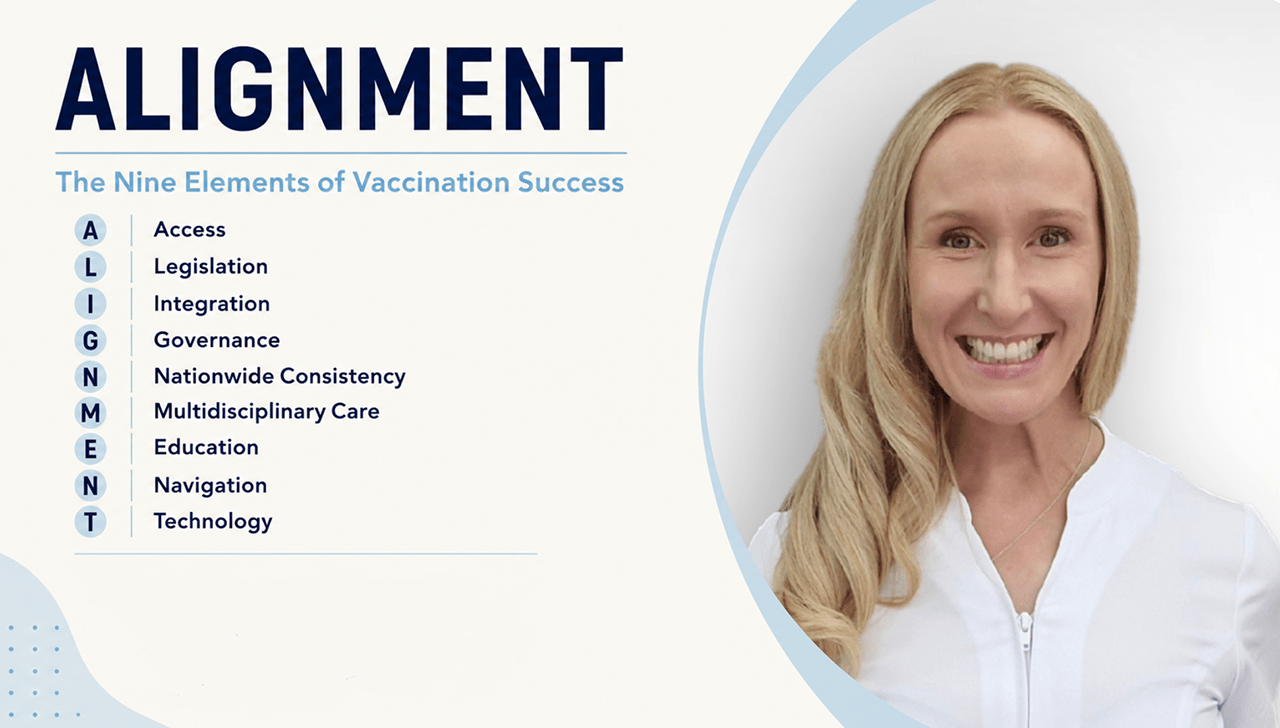
[post_content] => Pharmacy is now a major vaccination provider, but lifting uptake will depend on aligning policy, funding and legislation – as well as how effectively pharmacists embed vaccination into everyday care.
Speaking at the Communicable Diseases & Immunisation Conference 2026 last week, outgoing PSA inaugural Vaccination Ambassador Anna Theophilos MPS set out what it will take to expand pharmacist vaccination and close persistent gaps in access nationwide.
Pharmacists as vaccinators is no longer up for debate
More than a decade has passed since pharmacists first began administering influenza vaccines as part of a pilot program. Today, pharmacists can initiate and administer vaccines to protect patients against 25 vaccine-preventable diseases. Ms Theophilos said that pharmacists had proved themselves as vaccinators:
‘The true measure of success is no longer whether pharmacy can vaccinate. It's whether we can achieve full alignment between this extraordinary infrastructure and our public health goals.’
There’s more to access than physical location
Physical access has long been one of pharmacy's major strengths, with ‘more community pharmacies in Australia than Woolworths and McDonald's combined’, Ms Theophilos said.
But physical proximity doesn’t guarantee access to care.
 ‘Access is not simply about opening the door to another provider,’ she said. ‘True access is about removing every barrier between a patient and that provider.’
‘Access is not simply about opening the door to another provider,’ she said. ‘True access is about removing every barrier between a patient and that provider.’
There’s also more to access than remuneration
The introduction of the National Immunisation Program Vaccinations in Pharmacy (NIPVIP) in 2024 removed one of the most significant barriers – cost.
‘For years, pharmacists found themselves having difficult conversations with patients. The vaccine was free, but the administration fee wasn't,’ she said. ‘For many patients, that fee became the difference between vaccinating today and delaying vaccination altogether.’
‘State legislation must align with federal funding. It's as simple as that.'
Anna Theophilos MPS
The recent expansion of NIPVIP in this year’s federal budget to include children under 5 represents another step forward. However, differences in state and territory legislation continue to affect access to care.
‘Parents have openly told me that their younger children don't receive an influenza vaccination because they simply never get around to making a separate appointment with a GP,’ she said.
‘I can vaccinate their 6-year-old.I can vaccinate their 8-year-old. I can vaccinate their 10-year-old. But I can't vaccinate their 4-year-old, often the child at greatest risk.’
The result isn't just reduced access. It's confusion. And when healthcare becomes confusing, people delay it.
‘Alignment with the Australian Immunisation Handbook across all jurisdictions is overdue,’ Ms Theophilos said. ‘State legislation must align with federal funding. It's as simple as that.’
Vaccination isn’t yet standard care in every pharmacy. This must change
If anyone knows how to expand vaccination services, it’s Ms Theophilos. When she first took over her Melbourne-based community pharmacy in 2022, it was providing 200 vaccinations per year; now, the pharmacy administers almost 7,000.
How? integration.
‘Vaccination stopped being a service we offered and became part of the care we delivered,’ she said.
In practice, that means every member of the pharmacy team has a defined role; pharmacy assistants identify opportunities before a pharmacist is even involved.
‘A patient asks for Gastro-Stop because they're heading overseas next month? Before I even know they are in the pharmacy, they're being walked down to the consultation room for a Hepatitis A and Typhoid vaccination.’
By the time the pharmacist enters the consultation room, screening is complete, paperwork is done and the focus can be purely clinical.
‘Alignment of vaccination within your workflow, rather than alongside it as a separate service, is one of the most important drivers of vaccination success,’ Ms Theophilos said.
Consistency matters too
Patients often walk into a pharmacy seeking a vaccination only to be told the pharmacy doesn't offer vaccinations, or that the vaccinating pharmacist isn't available.
‘Imagine walking into a pharmacy with a prescription and being told, “Sorry, we don't dispense today.” It would be unthinkable,’ she said. ‘Yet we continue to accept this variability when it comes to vaccination.’
Pharmacy vaccination, she argued, has matured beyond being an optional service. ‘It must become a standard expectation of care.’
Making more powerful recommendations
Offering vaccination is one thing. But , clinical education is what turns a vaccination schedule into a strong health professional recommendation.
For example, when a patient says, ‘I've had eight COVID-19 shots – surely that's enough’, pharmacists can explain why boosters remain important for older adults. This includes discussing the risks associated with COVID-19 infection, including heart attack, stroke and myocarditis, and explaining that these risks are generally higher from the disease than from vaccination.
'Education turns eligibility into relevance. And relevance drives recommendations, which drives uptake,’ Ms Theophilos said.
Reaching thousands not hundreds
Technology is what then allows all of this to scale, enabling:

td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32424
[post_author] => 3410
[post_date] => 2026-06-22 14:44:11
[post_date_gmt] => 2026-06-22 04:44:11
[post_content] => New research has found that real-time prescription monitoring (RTPM) is changing prescribing behaviour – ultimately saving lives.
The study, led by Monash University researchers, is the first Australian research to examine the association between prescription drug monitoring program implementation and changes in multiple prescriber rates.
Key findings after SafeScript introduction (2019):
|

td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32421
[post_author] => 12503
[post_date] => 2026-06-22 14:24:10
[post_date_gmt] => 2026-06-22 04:24:10
[post_content] =>
The PSA has opened Expressions of Interest (EOIs) for its first PSA Harm Reduction Champion, who will act as a national spokesperson – advocating for and supporting PSA’s work in policy, professional practice, and community engagement.
EOIs are sought from passionate pharmacists looking to do more to support patients accessing harm reduction services such as opioid dependence therapy (ODT), the administration of long-acting injectable buprenorphine, naloxone access, and needle and syringe programs.
Supported by a grant from Camurus, the PSA Harm Reduction Champion role aims to elevate pharmacist leadership in harm reduction and strengthen the profession’s role in improving access to care, reducing stigma and supporting safer health outcomes for the community.
PSA National President, Professor Mark Naunton MPS, said pharmacists play a critical role in ensuring the safe provision of harm reduction services on the frontline.
‘Pharmacists have an important role to play in harm reduction, through improving access to essential services such as ODT, take-home naloxone, and needle and syringe programs, but there is still more to be done to support the equitable access to these services,’ Professor Naunton said.
‘This is why we’re looking for a pharmacist who is making a real impact in their community, and ready to help lead the conversations, support their communities, and advocate for expanded access to care through the PSA Harm Reduction Champion initiative.
‘If this sounds like you, or someone you know, I encourage you to submit an EOI to become PSA’s first Harm Reduction Champion.’
Dr Annie Madden AO, Executive Director of Harm Reduction Australia, welcomed the PSA Harm Reduction Champion initiative as an important step in further strengthening pharmacists’ leadership in harm reduction.
‘Pharmacists play a vital role in improving access to harm reduction services, and this new advocacy approach will hopefully inspire more pharmacists to engage in this highly rewarding area of practice, further expanding access to services that reduce harm, save lives, and strengthen the health and wellbeing of communities across Australia.’
EOIs are open to all PSA members and close 30 June 2026.
Pharmacists interested in becoming the 2026 PSA Harm Reduction Champion can submit an EOI at: https://forms.office.com/

td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32376
[post_author] => 12590
[post_date] => 2026-06-16 17:38:03
[post_date_gmt] => 2026-06-16 07:38:03
[post_content] => While effective for many, smoking cessation strategies are not a one-size-fits-all approach.
Nicotine replacement therapy (NRT) aims to reduce cravings and withdrawal symptoms by delivering nicotine in a safer, slower release form than smoking.1,2 NRT is a first-line pharmacotherapy for smoking cessation if clinically appropriate, and is shown to be effective.3 Pharmacists can also help to reframe past quit attempts as valuable learning opportunities for patients.
Here are some key NRT troubleshooting considerations pharmacists should consider.
Is the dose high enough?
NRT is safer than smoking and has low addictive potential.4 It is often under-dosed in practice, which can undermine a patient’s confidence in treatment.2,4,5 Patients may receive an inadequate dose, use NRT inconsistently or discontinue treatment prematurely.
When used at optimal doses, evidence shows NRT increases quit success.2 Pharmacists should use a nicotine dependence assessment tool (e.g. Quit Centre’s NRT tool) for dosage guidance and encourage proactive use of faster-acting NRT in anticipation of a trigger or cravings. Patients who have stopped smoking after an initial 8-week course of NRT may also benefit from a follow-up course.4
For some patients, combination NRT (patch and faster-acting form) may be appropriate. Combination NRT is equally as effective as varenicline and more effective than NRT monotherapy for smoking cessation.4
Does technique impact efficacy?
Incorrect use of NRT may lead to reduced nicotine absorption, increased adverse effects and reduced confidence in treatment.
To ensure maximum absorption, counselling points could include:

td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32348
[post_author] => 12503
[post_date] => 2026-06-15 09:23:36
[post_date_gmt] => 2026-06-14 23:23:36
[post_content] => Meet the award-winning pharmacists recognised for their exceptional contributions to patients, communities and the profession.
The PSA acknowledged the outstanding contributions, leadership, and dedication of the five pharmacists who were recognised at the PSA Victorian Pharmacist Awards.
The 2026 award recipients are:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32437
[post_author] => 3410
[post_date] => 2026-06-24 11:53:45
[post_date_gmt] => 2026-06-24 01:53:45
[post_content] => Pharmacy is now a major vaccination provider, but lifting uptake will depend on aligning policy, funding and legislation – as well as how effectively pharmacists embed vaccination into everyday care.
Speaking at the Communicable Diseases & Immunisation Conference 2026 last week, outgoing PSA inaugural Vaccination Ambassador Anna Theophilos MPS set out what it will take to expand pharmacist vaccination and close persistent gaps in access nationwide.
Pharmacists as vaccinators is no longer up for debate
More than a decade has passed since pharmacists first began administering influenza vaccines as part of a pilot program. Today, pharmacists can initiate and administer vaccines to protect patients against 25 vaccine-preventable diseases. Ms Theophilos said that pharmacists had proved themselves as vaccinators:
‘The true measure of success is no longer whether pharmacy can vaccinate. It's whether we can achieve full alignment between this extraordinary infrastructure and our public health goals.’
There’s more to access than physical location
Physical access has long been one of pharmacy's major strengths, with ‘more community pharmacies in Australia than Woolworths and McDonald's combined’, Ms Theophilos said.
But physical proximity doesn’t guarantee access to care.
‘Access is not simply about opening the door to another provider,’ she said. ‘True access is about removing every barrier between a patient and that provider.’
There’s also more to access than remuneration
The introduction of the National Immunisation Program Vaccinations in Pharmacy (NIPVIP) in 2024 removed one of the most significant barriers – cost.
‘For years, pharmacists found themselves having difficult conversations with patients. The vaccine was free, but the administration fee wasn't,’ she said. ‘For many patients, that fee became the difference between vaccinating today and delaying vaccination altogether.’
‘State legislation must align with federal funding. It's as simple as that.'
Anna Theophilos MPS
The recent expansion of NIPVIP in this year’s federal budget to include children under 5 represents another step forward. However, differences in state and territory legislation continue to affect access to care.
‘Parents have openly told me that their younger children don't receive an influenza vaccination because they simply never get around to making a separate appointment with a GP,’ she said.
‘I can vaccinate their 6-year-old.I can vaccinate their 8-year-old. I can vaccinate their 10-year-old. But I can't vaccinate their 4-year-old, often the child at greatest risk.’
The result isn't just reduced access. It's confusion. And when healthcare becomes confusing, people delay it.
‘Alignment with the Australian Immunisation Handbook across all jurisdictions is overdue,’ Ms Theophilos said. ‘State legislation must align with federal funding. It's as simple as that.’
Vaccination isn’t yet standard care in every pharmacy. This must change
If anyone knows how to expand vaccination services, it’s Ms Theophilos. When she first took over her Melbourne-based community pharmacy in 2022, it was providing 200 vaccinations per year; now, the pharmacy administers almost 7,000.
How? integration.
‘Vaccination stopped being a service we offered and became part of the care we delivered,’ she said.
In practice, that means every member of the pharmacy team has a defined role; pharmacy assistants identify opportunities before a pharmacist is even involved.
‘A patient asks for Gastro-Stop because they're heading overseas next month? Before I even know they are in the pharmacy, they're being walked down to the consultation room for a Hepatitis A and Typhoid vaccination.’
By the time the pharmacist enters the consultation room, screening is complete, paperwork is done and the focus can be purely clinical.
‘Alignment of vaccination within your workflow, rather than alongside it as a separate service, is one of the most important drivers of vaccination success,’ Ms Theophilos said.
Consistency matters too
Patients often walk into a pharmacy seeking a vaccination only to be told the pharmacy doesn't offer vaccinations, or that the vaccinating pharmacist isn't available.
‘Imagine walking into a pharmacy with a prescription and being told, “Sorry, we don't dispense today.” It would be unthinkable,’ she said. ‘Yet we continue to accept this variability when it comes to vaccination.’
Pharmacy vaccination, she argued, has matured beyond being an optional service. ‘It must become a standard expectation of care.’
Making more powerful recommendations
Offering vaccination is one thing. But , clinical education is what turns a vaccination schedule into a strong health professional recommendation.
For example, when a patient says, ‘I've had eight COVID-19 shots – surely that's enough’, pharmacists can explain why boosters remain important for older adults. This includes discussing the risks associated with COVID-19 infection, including heart attack, stroke and myocarditis, and explaining that these risks are generally higher from the disease than from vaccination.
'Education turns eligibility into relevance. And relevance drives recommendations, which drives uptake,’ Ms Theophilos said.
Reaching thousands not hundreds
Technology is what then allows all of this to scale, enabling:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32424
[post_author] => 3410
[post_date] => 2026-06-22 14:44:11
[post_date_gmt] => 2026-06-22 04:44:11
[post_content] => New research has found that real-time prescription monitoring (RTPM) is changing prescribing behaviour – ultimately saving lives.
The study, led by Monash University researchers, is the first Australian research to examine the association between prescription drug monitoring program implementation and changes in multiple prescriber rates.
Key findings after SafeScript introduction (2019):
|
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32421
[post_author] => 12503
[post_date] => 2026-06-22 14:24:10
[post_date_gmt] => 2026-06-22 04:24:10
[post_content] =>
The PSA has opened Expressions of Interest (EOIs) for its first PSA Harm Reduction Champion, who will act as a national spokesperson – advocating for and supporting PSA’s work in policy, professional practice, and community engagement.
EOIs are sought from passionate pharmacists looking to do more to support patients accessing harm reduction services such as opioid dependence therapy (ODT), the administration of long-acting injectable buprenorphine, naloxone access, and needle and syringe programs.
Supported by a grant from Camurus, the PSA Harm Reduction Champion role aims to elevate pharmacist leadership in harm reduction and strengthen the profession’s role in improving access to care, reducing stigma and supporting safer health outcomes for the community.
PSA National President, Professor Mark Naunton MPS, said pharmacists play a critical role in ensuring the safe provision of harm reduction services on the frontline.
‘Pharmacists have an important role to play in harm reduction, through improving access to essential services such as ODT, take-home naloxone, and needle and syringe programs, but there is still more to be done to support the equitable access to these services,’ Professor Naunton said.
‘This is why we’re looking for a pharmacist who is making a real impact in their community, and ready to help lead the conversations, support their communities, and advocate for expanded access to care through the PSA Harm Reduction Champion initiative.
‘If this sounds like you, or someone you know, I encourage you to submit an EOI to become PSA’s first Harm Reduction Champion.’
Dr Annie Madden AO, Executive Director of Harm Reduction Australia, welcomed the PSA Harm Reduction Champion initiative as an important step in further strengthening pharmacists’ leadership in harm reduction.
‘Pharmacists play a vital role in improving access to harm reduction services, and this new advocacy approach will hopefully inspire more pharmacists to engage in this highly rewarding area of practice, further expanding access to services that reduce harm, save lives, and strengthen the health and wellbeing of communities across Australia.’
EOIs are open to all PSA members and close 30 June 2026.
Pharmacists interested in becoming the 2026 PSA Harm Reduction Champion can submit an EOI at: https://forms.office.com/
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32376
[post_author] => 12590
[post_date] => 2026-06-16 17:38:03
[post_date_gmt] => 2026-06-16 07:38:03
[post_content] => While effective for many, smoking cessation strategies are not a one-size-fits-all approach.
Nicotine replacement therapy (NRT) aims to reduce cravings and withdrawal symptoms by delivering nicotine in a safer, slower release form than smoking.1,2 NRT is a first-line pharmacotherapy for smoking cessation if clinically appropriate, and is shown to be effective.3 Pharmacists can also help to reframe past quit attempts as valuable learning opportunities for patients.
Here are some key NRT troubleshooting considerations pharmacists should consider.
Is the dose high enough?
NRT is safer than smoking and has low addictive potential.4 It is often under-dosed in practice, which can undermine a patient’s confidence in treatment.2,4,5 Patients may receive an inadequate dose, use NRT inconsistently or discontinue treatment prematurely.
When used at optimal doses, evidence shows NRT increases quit success.2 Pharmacists should use a nicotine dependence assessment tool (e.g. Quit Centre’s NRT tool) for dosage guidance and encourage proactive use of faster-acting NRT in anticipation of a trigger or cravings. Patients who have stopped smoking after an initial 8-week course of NRT may also benefit from a follow-up course.4
For some patients, combination NRT (patch and faster-acting form) may be appropriate. Combination NRT is equally as effective as varenicline and more effective than NRT monotherapy for smoking cessation.4
Does technique impact efficacy?
Incorrect use of NRT may lead to reduced nicotine absorption, increased adverse effects and reduced confidence in treatment.
To ensure maximum absorption, counselling points could include:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32348
[post_author] => 12503
[post_date] => 2026-06-15 09:23:36
[post_date_gmt] => 2026-06-14 23:23:36
[post_content] => Meet the award-winning pharmacists recognised for their exceptional contributions to patients, communities and the profession.
The PSA acknowledged the outstanding contributions, leadership, and dedication of the five pharmacists who were recognised at the PSA Victorian Pharmacist Awards.
The 2026 award recipients are:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32437
[post_author] => 3410
[post_date] => 2026-06-24 11:53:45
[post_date_gmt] => 2026-06-24 01:53:45
[post_content] => Pharmacy is now a major vaccination provider, but lifting uptake will depend on aligning policy, funding and legislation – as well as how effectively pharmacists embed vaccination into everyday care.
Speaking at the Communicable Diseases & Immunisation Conference 2026 last week, outgoing PSA inaugural Vaccination Ambassador Anna Theophilos MPS set out what it will take to expand pharmacist vaccination and close persistent gaps in access nationwide.
Pharmacists as vaccinators is no longer up for debate
More than a decade has passed since pharmacists first began administering influenza vaccines as part of a pilot program. Today, pharmacists can initiate and administer vaccines to protect patients against 25 vaccine-preventable diseases. Ms Theophilos said that pharmacists had proved themselves as vaccinators:
‘The true measure of success is no longer whether pharmacy can vaccinate. It's whether we can achieve full alignment between this extraordinary infrastructure and our public health goals.’
There’s more to access than physical location
Physical access has long been one of pharmacy's major strengths, with ‘more community pharmacies in Australia than Woolworths and McDonald's combined’, Ms Theophilos said.
But physical proximity doesn’t guarantee access to care.
‘Access is not simply about opening the door to another provider,’ she said. ‘True access is about removing every barrier between a patient and that provider.’
There’s also more to access than remuneration
The introduction of the National Immunisation Program Vaccinations in Pharmacy (NIPVIP) in 2024 removed one of the most significant barriers – cost.
‘For years, pharmacists found themselves having difficult conversations with patients. The vaccine was free, but the administration fee wasn't,’ she said. ‘For many patients, that fee became the difference between vaccinating today and delaying vaccination altogether.’
‘State legislation must align with federal funding. It's as simple as that.'
Anna Theophilos MPS
The recent expansion of NIPVIP in this year’s federal budget to include children under 5 represents another step forward. However, differences in state and territory legislation continue to affect access to care.
‘Parents have openly told me that their younger children don't receive an influenza vaccination because they simply never get around to making a separate appointment with a GP,’ she said.
‘I can vaccinate their 6-year-old.I can vaccinate their 8-year-old. I can vaccinate their 10-year-old. But I can't vaccinate their 4-year-old, often the child at greatest risk.’
The result isn't just reduced access. It's confusion. And when healthcare becomes confusing, people delay it.
‘Alignment with the Australian Immunisation Handbook across all jurisdictions is overdue,’ Ms Theophilos said. ‘State legislation must align with federal funding. It's as simple as that.’
Vaccination isn’t yet standard care in every pharmacy. This must change
If anyone knows how to expand vaccination services, it’s Ms Theophilos. When she first took over her Melbourne-based community pharmacy in 2022, it was providing 200 vaccinations per year; now, the pharmacy administers almost 7,000.
How? integration.
‘Vaccination stopped being a service we offered and became part of the care we delivered,’ she said.
In practice, that means every member of the pharmacy team has a defined role; pharmacy assistants identify opportunities before a pharmacist is even involved.
‘A patient asks for Gastro-Stop because they're heading overseas next month? Before I even know they are in the pharmacy, they're being walked down to the consultation room for a Hepatitis A and Typhoid vaccination.’
By the time the pharmacist enters the consultation room, screening is complete, paperwork is done and the focus can be purely clinical.
‘Alignment of vaccination within your workflow, rather than alongside it as a separate service, is one of the most important drivers of vaccination success,’ Ms Theophilos said.
Consistency matters too
Patients often walk into a pharmacy seeking a vaccination only to be told the pharmacy doesn't offer vaccinations, or that the vaccinating pharmacist isn't available.
‘Imagine walking into a pharmacy with a prescription and being told, “Sorry, we don't dispense today.” It would be unthinkable,’ she said. ‘Yet we continue to accept this variability when it comes to vaccination.’
Pharmacy vaccination, she argued, has matured beyond being an optional service. ‘It must become a standard expectation of care.’
Making more powerful recommendations
Offering vaccination is one thing. But , clinical education is what turns a vaccination schedule into a strong health professional recommendation.
For example, when a patient says, ‘I've had eight COVID-19 shots – surely that's enough’, pharmacists can explain why boosters remain important for older adults. This includes discussing the risks associated with COVID-19 infection, including heart attack, stroke and myocarditis, and explaining that these risks are generally higher from the disease than from vaccination.
'Education turns eligibility into relevance. And relevance drives recommendations, which drives uptake,’ Ms Theophilos said.
Reaching thousands not hundreds
Technology is what then allows all of this to scale, enabling:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32424
[post_author] => 3410
[post_date] => 2026-06-22 14:44:11
[post_date_gmt] => 2026-06-22 04:44:11
[post_content] => New research has found that real-time prescription monitoring (RTPM) is changing prescribing behaviour – ultimately saving lives.
The study, led by Monash University researchers, is the first Australian research to examine the association between prescription drug monitoring program implementation and changes in multiple prescriber rates.
Key findings after SafeScript introduction (2019):
|
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32421
[post_author] => 12503
[post_date] => 2026-06-22 14:24:10
[post_date_gmt] => 2026-06-22 04:24:10
[post_content] =>
The PSA has opened Expressions of Interest (EOIs) for its first PSA Harm Reduction Champion, who will act as a national spokesperson – advocating for and supporting PSA’s work in policy, professional practice, and community engagement.
EOIs are sought from passionate pharmacists looking to do more to support patients accessing harm reduction services such as opioid dependence therapy (ODT), the administration of long-acting injectable buprenorphine, naloxone access, and needle and syringe programs.
Supported by a grant from Camurus, the PSA Harm Reduction Champion role aims to elevate pharmacist leadership in harm reduction and strengthen the profession’s role in improving access to care, reducing stigma and supporting safer health outcomes for the community.
PSA National President, Professor Mark Naunton MPS, said pharmacists play a critical role in ensuring the safe provision of harm reduction services on the frontline.
‘Pharmacists have an important role to play in harm reduction, through improving access to essential services such as ODT, take-home naloxone, and needle and syringe programs, but there is still more to be done to support the equitable access to these services,’ Professor Naunton said.
‘This is why we’re looking for a pharmacist who is making a real impact in their community, and ready to help lead the conversations, support their communities, and advocate for expanded access to care through the PSA Harm Reduction Champion initiative.
‘If this sounds like you, or someone you know, I encourage you to submit an EOI to become PSA’s first Harm Reduction Champion.’
Dr Annie Madden AO, Executive Director of Harm Reduction Australia, welcomed the PSA Harm Reduction Champion initiative as an important step in further strengthening pharmacists’ leadership in harm reduction.
‘Pharmacists play a vital role in improving access to harm reduction services, and this new advocacy approach will hopefully inspire more pharmacists to engage in this highly rewarding area of practice, further expanding access to services that reduce harm, save lives, and strengthen the health and wellbeing of communities across Australia.’
EOIs are open to all PSA members and close 30 June 2026.
Pharmacists interested in becoming the 2026 PSA Harm Reduction Champion can submit an EOI at: https://forms.office.com/
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32376
[post_author] => 12590
[post_date] => 2026-06-16 17:38:03
[post_date_gmt] => 2026-06-16 07:38:03
[post_content] => While effective for many, smoking cessation strategies are not a one-size-fits-all approach.
Nicotine replacement therapy (NRT) aims to reduce cravings and withdrawal symptoms by delivering nicotine in a safer, slower release form than smoking.1,2 NRT is a first-line pharmacotherapy for smoking cessation if clinically appropriate, and is shown to be effective.3 Pharmacists can also help to reframe past quit attempts as valuable learning opportunities for patients.
Here are some key NRT troubleshooting considerations pharmacists should consider.
Is the dose high enough?
NRT is safer than smoking and has low addictive potential.4 It is often under-dosed in practice, which can undermine a patient’s confidence in treatment.2,4,5 Patients may receive an inadequate dose, use NRT inconsistently or discontinue treatment prematurely.
When used at optimal doses, evidence shows NRT increases quit success.2 Pharmacists should use a nicotine dependence assessment tool (e.g. Quit Centre’s NRT tool) for dosage guidance and encourage proactive use of faster-acting NRT in anticipation of a trigger or cravings. Patients who have stopped smoking after an initial 8-week course of NRT may also benefit from a follow-up course.4
For some patients, combination NRT (patch and faster-acting form) may be appropriate. Combination NRT is equally as effective as varenicline and more effective than NRT monotherapy for smoking cessation.4
Does technique impact efficacy?
Incorrect use of NRT may lead to reduced nicotine absorption, increased adverse effects and reduced confidence in treatment.
To ensure maximum absorption, counselling points could include:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32348
[post_author] => 12503
[post_date] => 2026-06-15 09:23:36
[post_date_gmt] => 2026-06-14 23:23:36
[post_content] => Meet the award-winning pharmacists recognised for their exceptional contributions to patients, communities and the profession.
The PSA acknowledged the outstanding contributions, leadership, and dedication of the five pharmacists who were recognised at the PSA Victorian Pharmacist Awards.
The 2026 award recipients are:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32437
[post_author] => 3410
[post_date] => 2026-06-24 11:53:45
[post_date_gmt] => 2026-06-24 01:53:45
[post_content] => Pharmacy is now a major vaccination provider, but lifting uptake will depend on aligning policy, funding and legislation – as well as how effectively pharmacists embed vaccination into everyday care.
Speaking at the Communicable Diseases & Immunisation Conference 2026 last week, outgoing PSA inaugural Vaccination Ambassador Anna Theophilos MPS set out what it will take to expand pharmacist vaccination and close persistent gaps in access nationwide.
Pharmacists as vaccinators is no longer up for debate
More than a decade has passed since pharmacists first began administering influenza vaccines as part of a pilot program. Today, pharmacists can initiate and administer vaccines to protect patients against 25 vaccine-preventable diseases. Ms Theophilos said that pharmacists had proved themselves as vaccinators:
‘The true measure of success is no longer whether pharmacy can vaccinate. It's whether we can achieve full alignment between this extraordinary infrastructure and our public health goals.’
There’s more to access than physical location
Physical access has long been one of pharmacy's major strengths, with ‘more community pharmacies in Australia than Woolworths and McDonald's combined’, Ms Theophilos said.
But physical proximity doesn’t guarantee access to care.
‘Access is not simply about opening the door to another provider,’ she said. ‘True access is about removing every barrier between a patient and that provider.’
There’s also more to access than remuneration
The introduction of the National Immunisation Program Vaccinations in Pharmacy (NIPVIP) in 2024 removed one of the most significant barriers – cost.
‘For years, pharmacists found themselves having difficult conversations with patients. The vaccine was free, but the administration fee wasn't,’ she said. ‘For many patients, that fee became the difference between vaccinating today and delaying vaccination altogether.’
‘State legislation must align with federal funding. It's as simple as that.'
Anna Theophilos MPS
The recent expansion of NIPVIP in this year’s federal budget to include children under 5 represents another step forward. However, differences in state and territory legislation continue to affect access to care.
‘Parents have openly told me that their younger children don't receive an influenza vaccination because they simply never get around to making a separate appointment with a GP,’ she said.
‘I can vaccinate their 6-year-old.I can vaccinate their 8-year-old. I can vaccinate their 10-year-old. But I can't vaccinate their 4-year-old, often the child at greatest risk.’
The result isn't just reduced access. It's confusion. And when healthcare becomes confusing, people delay it.
‘Alignment with the Australian Immunisation Handbook across all jurisdictions is overdue,’ Ms Theophilos said. ‘State legislation must align with federal funding. It's as simple as that.’
Vaccination isn’t yet standard care in every pharmacy. This must change
If anyone knows how to expand vaccination services, it’s Ms Theophilos. When she first took over her Melbourne-based community pharmacy in 2022, it was providing 200 vaccinations per year; now, the pharmacy administers almost 7,000.
How? integration.
‘Vaccination stopped being a service we offered and became part of the care we delivered,’ she said.
In practice, that means every member of the pharmacy team has a defined role; pharmacy assistants identify opportunities before a pharmacist is even involved.
‘A patient asks for Gastro-Stop because they're heading overseas next month? Before I even know they are in the pharmacy, they're being walked down to the consultation room for a Hepatitis A and Typhoid vaccination.’
By the time the pharmacist enters the consultation room, screening is complete, paperwork is done and the focus can be purely clinical.
‘Alignment of vaccination within your workflow, rather than alongside it as a separate service, is one of the most important drivers of vaccination success,’ Ms Theophilos said.
Consistency matters too
Patients often walk into a pharmacy seeking a vaccination only to be told the pharmacy doesn't offer vaccinations, or that the vaccinating pharmacist isn't available.
‘Imagine walking into a pharmacy with a prescription and being told, “Sorry, we don't dispense today.” It would be unthinkable,’ she said. ‘Yet we continue to accept this variability when it comes to vaccination.’
Pharmacy vaccination, she argued, has matured beyond being an optional service. ‘It must become a standard expectation of care.’
Making more powerful recommendations
Offering vaccination is one thing. But , clinical education is what turns a vaccination schedule into a strong health professional recommendation.
For example, when a patient says, ‘I've had eight COVID-19 shots – surely that's enough’, pharmacists can explain why boosters remain important for older adults. This includes discussing the risks associated with COVID-19 infection, including heart attack, stroke and myocarditis, and explaining that these risks are generally higher from the disease than from vaccination.
'Education turns eligibility into relevance. And relevance drives recommendations, which drives uptake,’ Ms Theophilos said.
Reaching thousands not hundreds
Technology is what then allows all of this to scale, enabling:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32424
[post_author] => 3410
[post_date] => 2026-06-22 14:44:11
[post_date_gmt] => 2026-06-22 04:44:11
[post_content] => New research has found that real-time prescription monitoring (RTPM) is changing prescribing behaviour – ultimately saving lives.
The study, led by Monash University researchers, is the first Australian research to examine the association between prescription drug monitoring program implementation and changes in multiple prescriber rates.
Key findings after SafeScript introduction (2019):
|
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32421
[post_author] => 12503
[post_date] => 2026-06-22 14:24:10
[post_date_gmt] => 2026-06-22 04:24:10
[post_content] =>
The PSA has opened Expressions of Interest (EOIs) for its first PSA Harm Reduction Champion, who will act as a national spokesperson – advocating for and supporting PSA’s work in policy, professional practice, and community engagement.
EOIs are sought from passionate pharmacists looking to do more to support patients accessing harm reduction services such as opioid dependence therapy (ODT), the administration of long-acting injectable buprenorphine, naloxone access, and needle and syringe programs.
Supported by a grant from Camurus, the PSA Harm Reduction Champion role aims to elevate pharmacist leadership in harm reduction and strengthen the profession’s role in improving access to care, reducing stigma and supporting safer health outcomes for the community.
PSA National President, Professor Mark Naunton MPS, said pharmacists play a critical role in ensuring the safe provision of harm reduction services on the frontline.
‘Pharmacists have an important role to play in harm reduction, through improving access to essential services such as ODT, take-home naloxone, and needle and syringe programs, but there is still more to be done to support the equitable access to these services,’ Professor Naunton said.
‘This is why we’re looking for a pharmacist who is making a real impact in their community, and ready to help lead the conversations, support their communities, and advocate for expanded access to care through the PSA Harm Reduction Champion initiative.
‘If this sounds like you, or someone you know, I encourage you to submit an EOI to become PSA’s first Harm Reduction Champion.’
Dr Annie Madden AO, Executive Director of Harm Reduction Australia, welcomed the PSA Harm Reduction Champion initiative as an important step in further strengthening pharmacists’ leadership in harm reduction.
‘Pharmacists play a vital role in improving access to harm reduction services, and this new advocacy approach will hopefully inspire more pharmacists to engage in this highly rewarding area of practice, further expanding access to services that reduce harm, save lives, and strengthen the health and wellbeing of communities across Australia.’
EOIs are open to all PSA members and close 30 June 2026.
Pharmacists interested in becoming the 2026 PSA Harm Reduction Champion can submit an EOI at: https://forms.office.com/
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32376
[post_author] => 12590
[post_date] => 2026-06-16 17:38:03
[post_date_gmt] => 2026-06-16 07:38:03
[post_content] => While effective for many, smoking cessation strategies are not a one-size-fits-all approach.
Nicotine replacement therapy (NRT) aims to reduce cravings and withdrawal symptoms by delivering nicotine in a safer, slower release form than smoking.1,2 NRT is a first-line pharmacotherapy for smoking cessation if clinically appropriate, and is shown to be effective.3 Pharmacists can also help to reframe past quit attempts as valuable learning opportunities for patients.
Here are some key NRT troubleshooting considerations pharmacists should consider.
Is the dose high enough?
NRT is safer than smoking and has low addictive potential.4 It is often under-dosed in practice, which can undermine a patient’s confidence in treatment.2,4,5 Patients may receive an inadequate dose, use NRT inconsistently or discontinue treatment prematurely.
When used at optimal doses, evidence shows NRT increases quit success.2 Pharmacists should use a nicotine dependence assessment tool (e.g. Quit Centre’s NRT tool) for dosage guidance and encourage proactive use of faster-acting NRT in anticipation of a trigger or cravings. Patients who have stopped smoking after an initial 8-week course of NRT may also benefit from a follow-up course.4
For some patients, combination NRT (patch and faster-acting form) may be appropriate. Combination NRT is equally as effective as varenicline and more effective than NRT monotherapy for smoking cessation.4
Does technique impact efficacy?
Incorrect use of NRT may lead to reduced nicotine absorption, increased adverse effects and reduced confidence in treatment.
To ensure maximum absorption, counselling points could include:
td_module_mega_menu Object
(
[post] => WP_Post Object
(
[ID] => 32348
[post_author] => 12503
[post_date] => 2026-06-15 09:23:36
[post_date_gmt] => 2026-06-14 23:23:36
[post_content] => Meet the award-winning pharmacists recognised for their exceptional contributions to patients, communities and the profession.
The PSA acknowledged the outstanding contributions, leadership, and dedication of the five pharmacists who were recognised at the PSA Victorian Pharmacist Awards.
The 2026 award recipients are:
The social highlight of the annual PSA conference is the Gala Dinner, and this year certainly did not disappoint.








Get your weekly dose of the news and research you need to help advance your practice.
Protected by Google reCAPTCHA v3.
Australian Pharmacist is the official journal for Pharmaceutical Society of Australia Ltd.


