


 Dan Malone MPS[/caption]
Dan Malone MPS[/caption]

 Tanya Maloney MPS[/caption]
Tanya Maloney MPS[/caption]
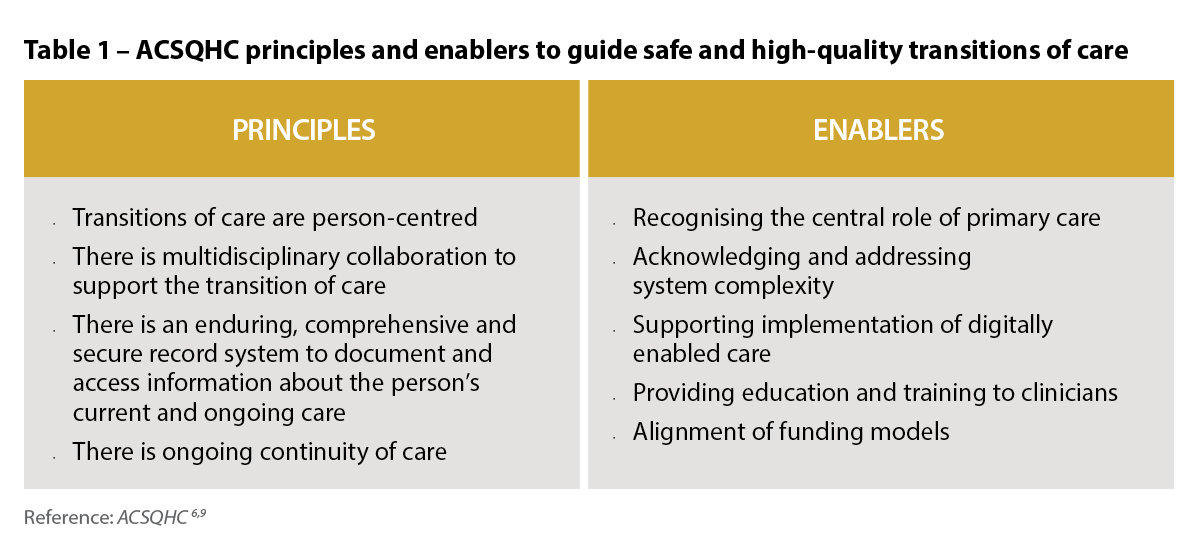 Australia’s priority actions to address medicines safety at transitions of care
Australia’s priority actions to address medicines safety at transitions of care
 CAL 6[/caption]
CAL 6[/caption]
 The old CAL 13[/caption]
[caption id="attachment_29337" align="aligncenter" width="189"]
The old CAL 13[/caption]
[caption id="attachment_29337" align="aligncenter" width="189"] The new CAL 13[/caption]
The new CAL 13[/caption]

Gunnedah-based Karen Carter FPS loves making a difference to patients’ health and wellbeing. She always knew she wanted to own a pharmacy. Now she has two .

Loan Pham MPS, a daughter of Vietnamese refugees, has spent 14 years at one pharmacy. She loves it so much, she’s hoping to buy it.
What set you on the path to a career in pharmacy?
Growing up in Sydney...

Pharmacists can help improve health outcomes for men, especially if they use communication skills to draw out those who don’t often visit doctors.

Jocelyn Watson, a PSA life member, was awarded an Order of Australia medal in January for services to Launceston and contributions to her church, horticultural society and her industry.

Hannah Knowles MPS loves being involved in every stage of a patients’ journey, an interest suited to her new role at a leading Brisbane hospital pharmacy.

Bernadette Cappello MPS has gone from community pharmacy, through the federal Department of Health to the World Health Organization in Geneva.

Medicine safety will be improved through empowering consumers and a combination of practice, policy and research initiatives.

More than 200,000 Australians currently live in aged care and the number grows each day. Optimising medicine safety is a crucial concern.

Mental health and substance use disorders are among the five leading causes of disease burden in Australia. What role can pharmacists play?

It took Bria Lacy five years to ‘find her voice’ but when she did, it was heard.
I was not expecting the overwhelming response I got,’ Ms Lacy said of the support she received after publishing her blog Finding My...

