

 Laura with her mum Michelle[/caption]
Laura with her mum Michelle[/caption]
 Nicolette Ellis MPS[/caption]
Nicolette Ellis MPS[/caption]

 For those at later stages of their lives, it’s important to avoid social isolation and to keep the brain active, she adds.
For those at later stages of their lives, it’s important to avoid social isolation and to keep the brain active, she adds.  Medicine administration frustrations can be avoided when dose time changes can be suggested.
Medicine administration frustrations can be avoided when dose time changes can be suggested. 

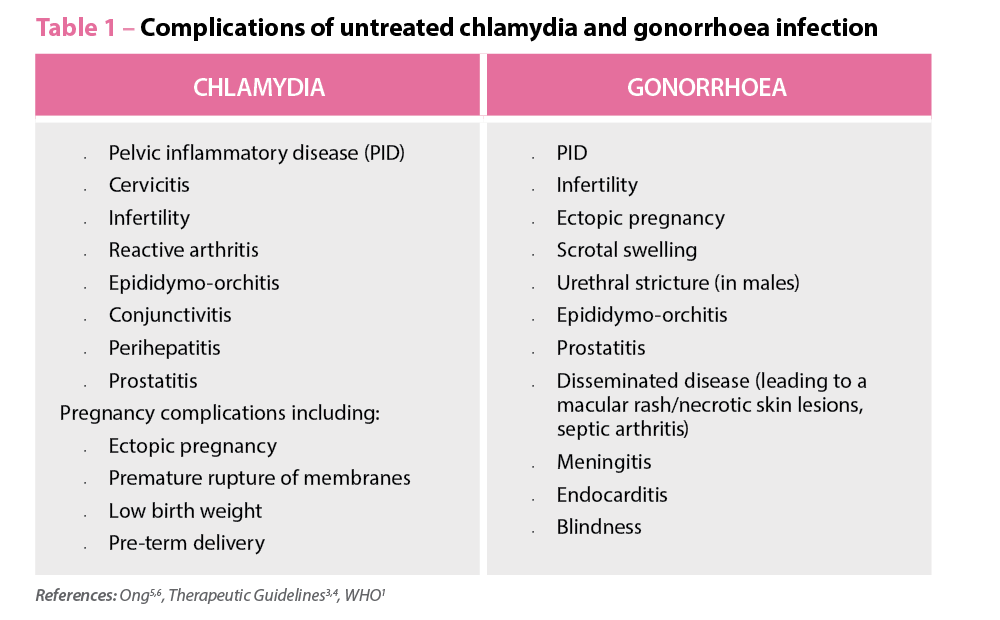 Diagnosis and differential diagnosis
Diagnosis and differential diagnosis  Gonococcal culture
Gonococcal culture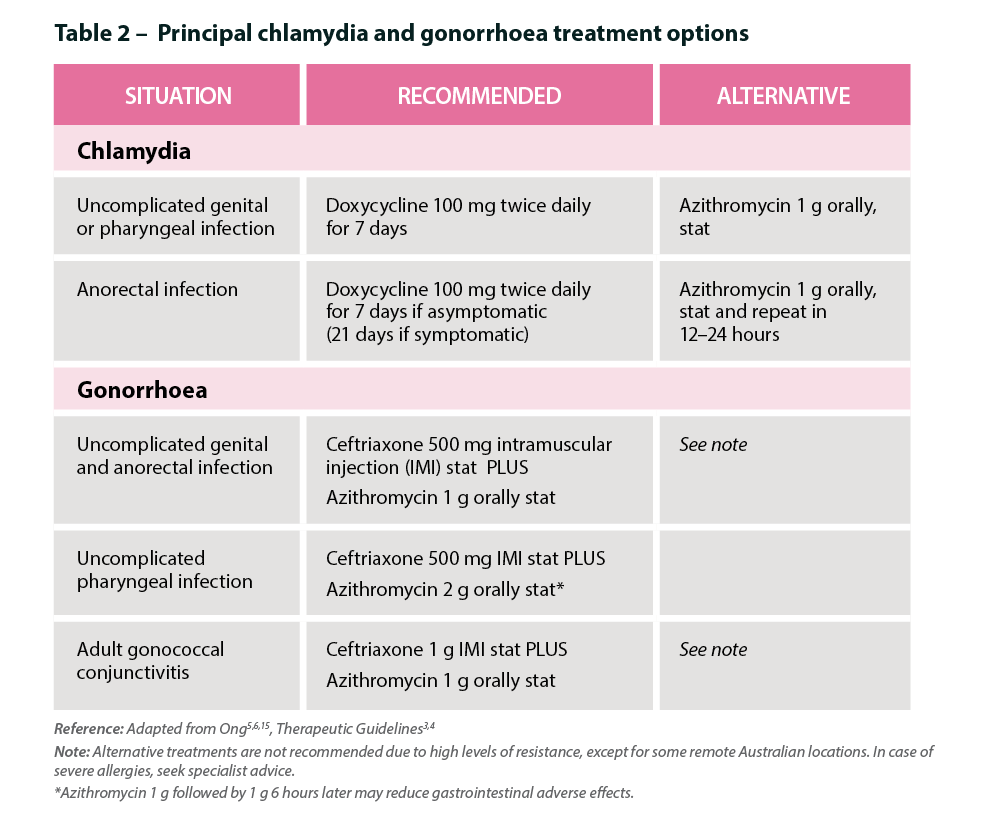 Prevention
Prevention 
 Dr Erica Stewart, Centenary Institute[/caption]
Dr Erica Stewart, Centenary Institute[/caption]

Community pharmacists in the Northern Territory are well-prepared for the national My Health Record (MHR) rollout, with nearly 70% of pharmacies either registered or awaiting registration processing.
Sam Keitaanpaa, Clinical Service Specialist at Country Wellness Group in Darwin, said the...

With new research showing current cardiovascular disease screening guidelines are missing younger at-risk Aboriginal people, a leading Aboriginal health specialist has highlighted the role pharmacists can play in preventative cardiac care.
The statement from National Aboriginal Community Controlled Health Organisation...

Australia’s cities hug the coast, but in rural and remote areas, sole pharmacists are providing communities with an essential service. Some may think it’s isolating, but many wouldn’t change a thing.
Around 1800 registered pharmacists work across outer regional to...

Pharmacist prescribing is ‘imminent’, says PSA National President Dr Shane Jackson. So what could that mean for you and your patients?
Pharmacists will have prescribing powers by 2020, predicts Shane Jackson.
‘Prescribing is an activity that is well within the...

Stoking a turf war between GPs and pharmacists will harm patient care, PSA National President Dr Shane Jackson has warned.
On Monday, the RACGP urged the public to avoid community pharmacy-run health checks, which RACGP Victoria chair Cameron Loy said...

WA-based hospital pharmacist Lauren Burton has been appointed as the new Early Career Pharmacist (ECP) Director of PSA, effective from 1 July 2018.
PSA National President Dr Shane Jackson said he was delighted to welcome Ms Burton to the...

Australian prescription dispensing volume is lower, but spending on PBS medicines has increased in the past two years, according to the Australian Institute of Health and Welfare (AIHW)’s biennial report on health information.
Gathered from government and non-government sources covering...

The Dose Administration Aids (DAA) program will be available to 70,000 more patients each year through community pharmacies, with the Federal Government announcing increased funding to expand the successful program.
PSA National President Dr Shane Jackson welcomed the increased availability...

Pharmacists within general practice is a positive step forward, but the exclusion from MBS Team Care arrangements in CDM items makes no sense.
After a long period of advocacy from PSA, and other medical groups including the AMA, the announcement...

Seeking greater remuneration and a different working life, some community pharmacists find themselves considering the leap to hospitals. So what do they need to know?
Transitioning from community to hospital pharmacy might seem like a daunting leap into the...

