

 Tanya Maloney MPS[/caption]
Tanya Maloney MPS[/caption]
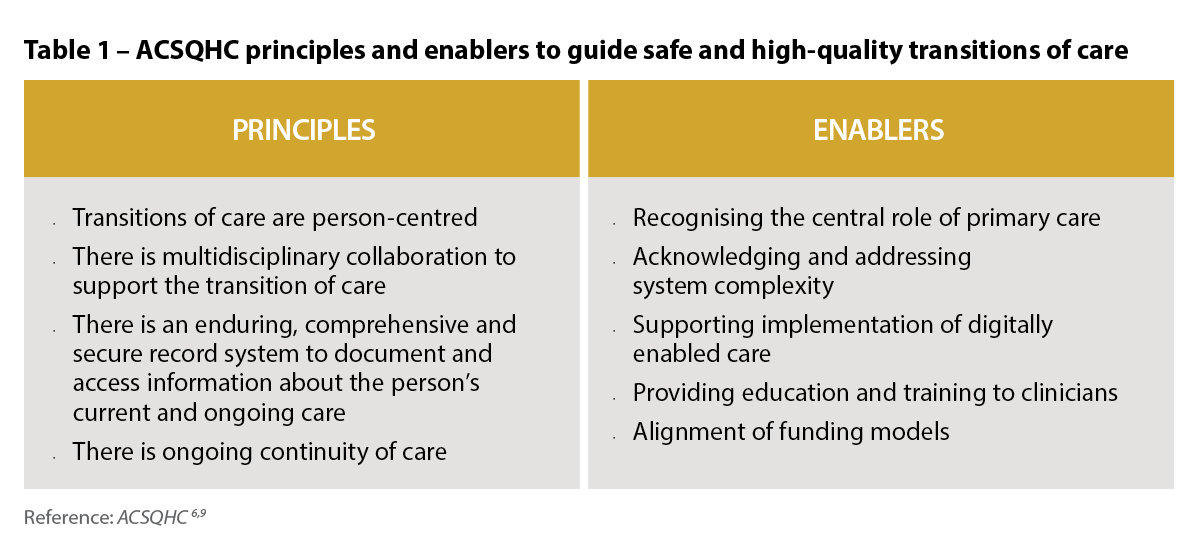 Australia’s priority actions to address medicines safety at transitions of care
Australia’s priority actions to address medicines safety at transitions of care
 CAL 6[/caption]
CAL 6[/caption]
 The old CAL 13[/caption]
[caption id="attachment_29337" align="aligncenter" width="189"]
The old CAL 13[/caption]
[caption id="attachment_29337" align="aligncenter" width="189"] The new CAL 13[/caption]
The new CAL 13[/caption]

 Revised CAL 18[/caption]
Revised CAL 18[/caption]


The new federal government last night delivered its 2022–23 ‘bread and butter’ Budget amid a growing cost-of-living crisis.

After the announcement of the AACP closure, Australian Pharmacist examines why PSA has and always will be the home of accreditation.

Pharmacists have been stranded without access to more than 730 PBS medicines struck off the Continued Dispensing initiative measure.

In this special episode of Pharmacy & Me, hosts Peter Guthrey and Hannah Knowles get to the heart of the issue, speaking with Ienaam and pharmacy owner Caroline Diamantis MPS about what needs to change when it comes to remuneration.

From honouring pharmacy excellence, providing emerging practice advice and celebrating innovation – the Queensland ATU didn’t disappoint.

The Pharmacy Board of Australia announced new work on pharmacist prescribing as NSW moves to initiate a UTI pharmacy prescribing pilot.

The new Deadly pharmacists foundation training course prepares pharmacists to work in Aboriginal Community-Controlled Health Organisations.

A new report revealed that there has been a significant reduction in antipsychotic dispensing in the past 5 years.

The National Asthma Council Australia has released a new guideline to upskill pharmacists in thunderstorm asthma management.

Like the great plague of 1665, the COVID-19 pandemic has demonstrated the value of pharmacists, and accelerated practice evolution.

