




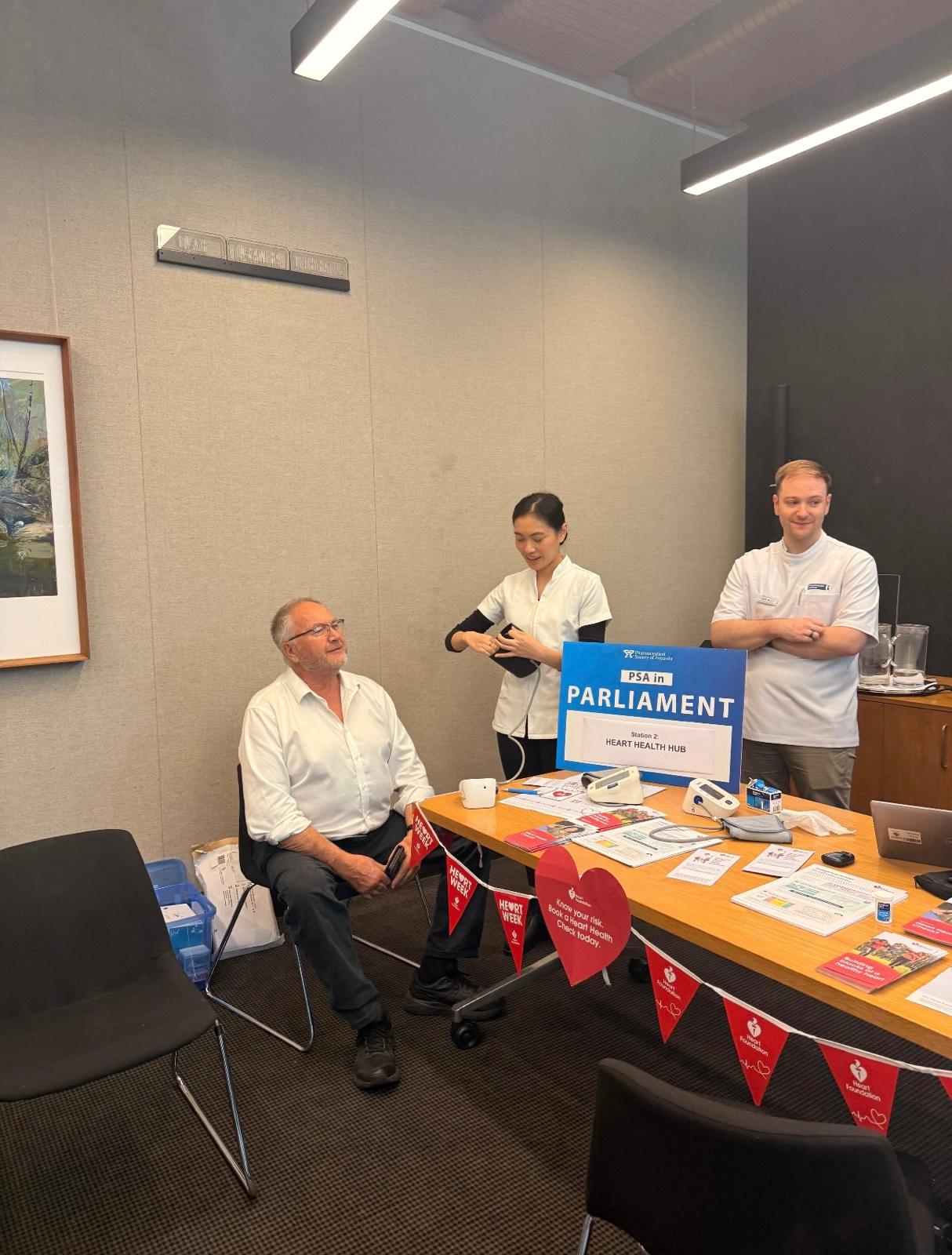
 A pop-up pharmacy clinic offering screening services after breakfast[/caption]
A pop-up pharmacy clinic offering screening services after breakfast[/caption]



The most-read stories of the year highlight where clinical practice, regulation and professional reform collided.
From sweeping Therapeutic Guidelines updates to unresolved scheduling decisions and award wage reform, these five stories captured pharmacists’ attention and reflected the pressures shaping practice...

New year, new policy and practice changes. Here’s what pharmacists will need to navigate from January.
In 2026, pharmacists can expect some changes to education, medicine costs and credentialing standards.
AP has rounded up the key changes pharmacists can expect from...

The Pharmaceutical Society of Australia (PSA) recently launched the PSA Standards for Continuing Professional Development (CPD) for Pharmacists, marking a new era for the accreditation of CPD activities for the pharmacy profession.
The launch of the PSA Standards follows the...

How pharmacists can flag SABA-only asthma patients, guide them to new therapies for optimal management, and correct inhaler technique.

Vaccines are most effective when administered using correct technique, including injection site positioning, and needle angle and length.

For years it seemed impossible to achieve, but markedly reducing chemical restraint is on its way.

Some pharmacists have recently pondered the possibility of administering cosmetic injectables such as Botox and dermal fillers, reaching out to PSA’s Pharmacist to Pharmacist Advice Line for guidance.
‘Now that pharmacists are injecting more medicines, and we have up-skilled to...

What to do if you send an electronic prescription to the wrong person.

With only two weeks before school resumes, now is the ideal time for pharmacists to help parents catch up with vaccinations for their children.

Turning informal advice into a structured consultation service: pharmacy-based travel health services take flight.
