



 Yvette Anderson MPS[/caption]
Yvette Anderson MPS[/caption]











Pharmacists in line for pay increase
The combination of an award wage rise and pay equity increase is set to deliver a meaningful lift in pharmacist remuneration.

Health leaders unite behind pharmacists in general practice
At the GP pharmacist symposium, leading health bodies have called for investment in general practice pharmacists to make medicine use safer.

How to manage ADHD medicine shortages
Australia's ADHD medicine supply has stabilised – for now. Here’s what pharmacists need to know before ADHD medicine shortages strike again.

Consultant pharmacist excellence awarded
Two pharmacists were honoured at PSA’s Consultant Pharmacist Conference (CPC26), held from 29–31 May 2026 on the Gold Coast.

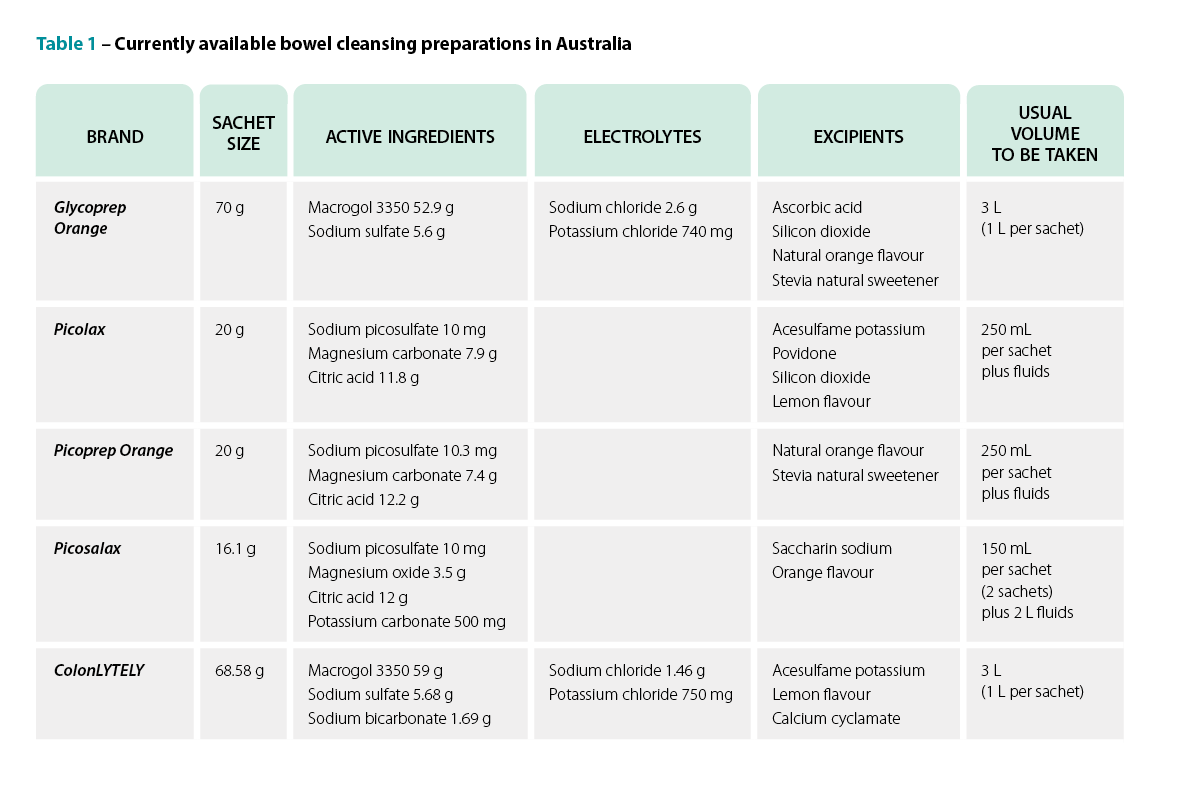
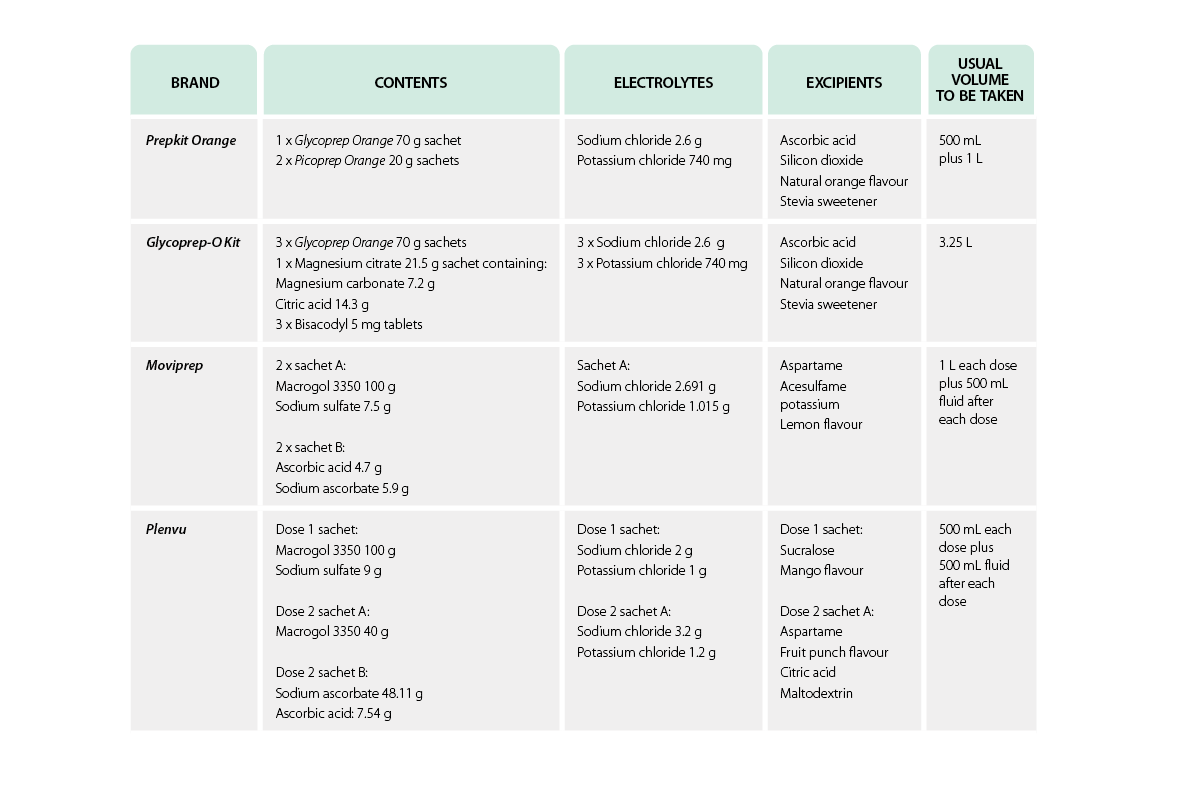
Optimising patient care in endoscopy and colonoscopy
Endoscopy and colonoscopy procedures are essential, in which adequate bowel preparation and patient counselling improve diagnostic accuracy.
Pharmacists in line for pay increase
The combination of an award wage rise and pay equity increase is set to deliver a meaningful lift in pharmacist remuneration.
Health leaders unite behind pharmacists in general practice
At the GP pharmacist symposium, leading health bodies have called for investment in general practice pharmacists to make medicine use safer.
How to manage ADHD medicine shortages
Australia's ADHD medicine supply has stabilised – for now. Here’s what pharmacists need to know before ADHD medicine shortages strike again.
Consultant pharmacist excellence awarded
Two pharmacists were honoured at PSA’s Consultant Pharmacist Conference (CPC26), held from 29–31 May 2026 on the Gold Coast.
Optimising patient care in endoscopy and colonoscopy
Endoscopy and colonoscopy procedures are essential, in which adequate bowel preparation and patient counselling improve diagnostic accuracy.
POPULAR
A cup of tea, a Bex and a good lie down

Immortalised in Australian slang, the analgesic phenacetin (used in Bex powder) is wrapped up in the development of the modern pharmaceutical industry and has...
Pfizer COVID-19 vaccine health hubs announced

The Federal Government is calling on community pharmacists to help vaccinate millions of Australians against COVID-19.
Landmark Australian study on oxycodone prescribing

Oxycodone is the most prescribed strong opioid in Australia. Yet little was known about its use and prescribing patterns – until now.
Triptans downscheduled to S3 medicines

Last year, the Therapeutic Goods Administration announced that certain triptans will be available over the counter in 2021.
New CAL D instruction for antibiotics

A new cautionary advisory label for antibiotics that will replace decades of advice to take the medicines ‘until all used’ or ‘until all taken’ will be released next year.
What impact will Wegovy have on the obesity epidemic?

The latest injectable glucagon-like peptide-1 receptor agonist, Wegovy, became available in Australia last week (5 August 2024).
